


Bile duct cancer
18 December 2023

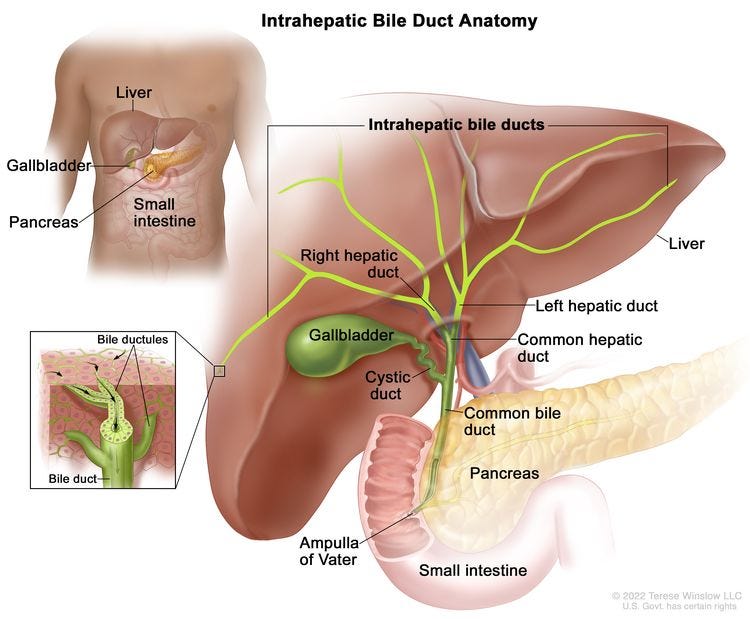
Bile duct cancer, also called cholangiocarcinoma, is typically discussed with liver cancer because the bile ducts originate in the liver. However, the cells of bile duct cancer resemble bile ducts and not liver cells, and these cancers behave differently from liver cell cancer (also called hepatocellular carcinoma).
Bile duct cancers are rare, with an estimated 8,000 new cases in the U.S. each year. They may be intrahepatic (i.e. originating within the liver), with an incidence of 1.5 cases per 100,000 U.S. population) or extrahepatic (i.e. originating from ducts outside of the liver, such as the common hepatic duct and the common bile duct) with an incidence of 1.0 cases per 100,000 population.
The overall 5 year relative survival for bile duct cancer is only 9-11%, among the lowest for all cancers (compared to 11% for pancreatic cancer, 20% for liver and esophageal cancer and 22% for lung cancer). It is 18-23% if the tumor is localized but only 2-3% if there are distant metastases.
A relative survival rate compares people with the same type and stage of cancer to people in the overall population. For example, if the 5-year relative survival rate for a specific stage of bile duct cancer (cholangiocarcinoma) is 30%, it means that people who have that cancer are, on average, about 30% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.


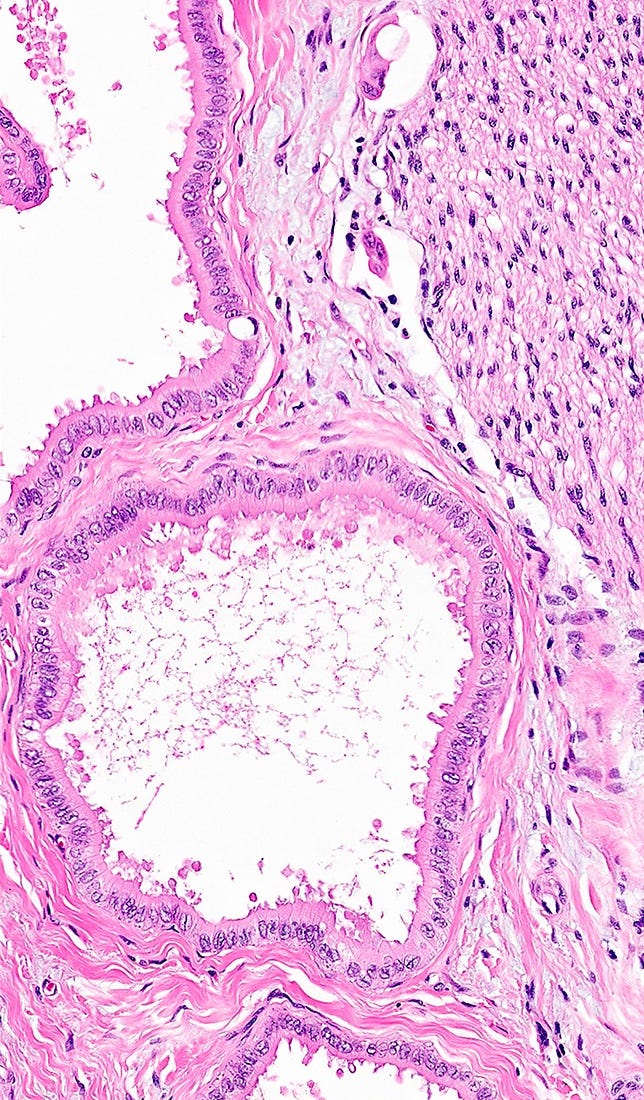
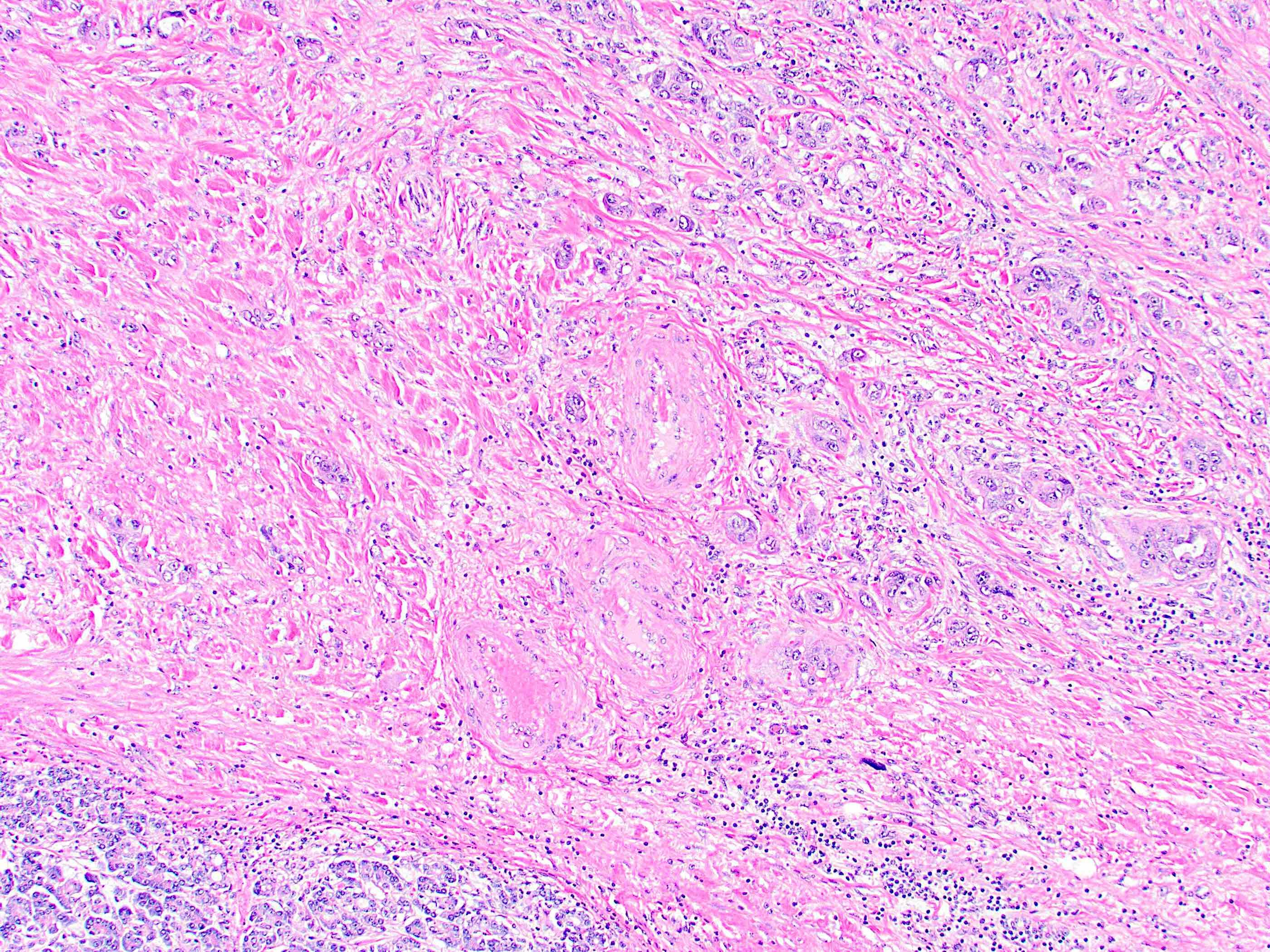
Microscopically, these tumors often contain well formed glands in a fibrous stroma. The glands exhibit atypia (i.e. abnormal nuclear features) and pleomorphism (variable nuclear features from cell to cell). Intrahepatic tumors commonly infiltrate between the normal liver cells. They may be composed of small ducts or large ducts.




What causes bile duct cancers?
A common risk factor for bile duct cancer is chronic inflammation of the biliary epithelium and bile stasis (i.e. the stalling of bile flow). However, in Western countries, 50% of cases have no identifiable risk factor.
Small duct tumors are often due to cirrhosis, nonalcoholic fatty liver disease / nonalcoholic steatohepatitis (NASH), hepatitis B or hepatitis C.
Large duct tumors are often due to:
Primary sclerosing cholangitis. These patients have a 10 - 20% lifetime risk of developing cholangiocarcinoma.
Hepatolithiasis (bile duct stones), particularly in Southeast Asia.
Liver flukes (parasites), specifically Opisthorchis viverrini and Clonorchis sinensis.
These parasites are associated with the daily consumption of raw freshwater and salt fermented fish in Thailand, causing repeated exposure to liver flukes and nitrosamine contaminated food. As a result, the incidence of cholangiocarcinoma is markedly elevated in Thailand (84.6 per 100,000) compared with Korea (7.4 per 100,000), Japan (2.8), Singapore (1.0) and Western countries (0.2 to 0.7) (Lim 2011).


Other risk factors are listed here.
How does chronic inflammation promote cancer?
Many of our biological networks are in a delicate balance between stimulating and dampening forces which is disturbed by continuous (chronic) activation of the inflammatory system.
Inflammatory networks are inherently more unstable than other physiologic networks because they rapidly initiate sophisticated repair processes in response to varied stimuli.
The inflammatory response consists of a coordinated program to facilitate tissue repair and kill foreign microorganisms (Pernick 2021 page 9). Physiologic triggers of inflammation simultaneously initiate the process of its resolution. As the trauma is repaired or the threat from foreign organisms subsides, the resolution process causes networks to revert to their initial states to prevent bystander damage to tissue. However, cancer risk factors trigger the inflammatory process with no simultaneous initiation of the resolution process, leading to persistent inflammation. This produces reactive oxygen and nitrogen species that damage DNA and also lessen the effectiveness of the immune system. These factors can promote genomic instability in other networks and further drive the malignant process unless some pro-resolution treatment is administered.
Researchers are studying the use of anti-inflammatory drugs to prevent and treat cancer. This is also part of our Strategic Plan to substantially reduce cancer deaths.
Index to Nat's blog on cancer and medicine
If you like these free essays, please share them with others.
Follow me on Substack or LinkedIn or through our Curing Cancer Newsletter (all are free). I have another blog on politics and abortion rights
Follow our Curing Cancer Network on LinkedIn and Twitter to view interesting images of cancer diagnoses, cancer essays and other cancer news.
Latest versions of our cancer essays:
American Code Against Cancer (how you can prevent cancer)
Email me at Nat@PathologyOutlines.com - Unfortunately, I cannot provide medical advice.
I also publish Notes at https://substack.com/note. Subscribers will automatically see my notes.
Other social media - Tribel: @nat385440b, Threads: npernickmich