


Cancer precursor project - breast cancer, part 6j
5 April 2025
This weekly medical blog is scientific, not political. I also publish a daily political blog. Skip any essays or parts of essays that you find too technical or are not interested in - I won’t be offended.
This essay is part of my cancer precursor project that discusses how different types of cancer arise. Part 6 discusses breast cancer. Click here for links to discussions for all 45 breast cancer types (some may be pending).
Part 6j discusses additional breast malignancies without known precursors, including metaplastic carcinoma and its variants metaplastic carcinoma: fibromatosis-like and metaplastic carcinoma: low grade adenosquamous, which are triple negative carcinomas. The variant metaplastic carcinoma: squamous cell carcinoma, which has a precursor (squamous dysplasia), was discussed here.
Metaplastic carcinoma of the breast
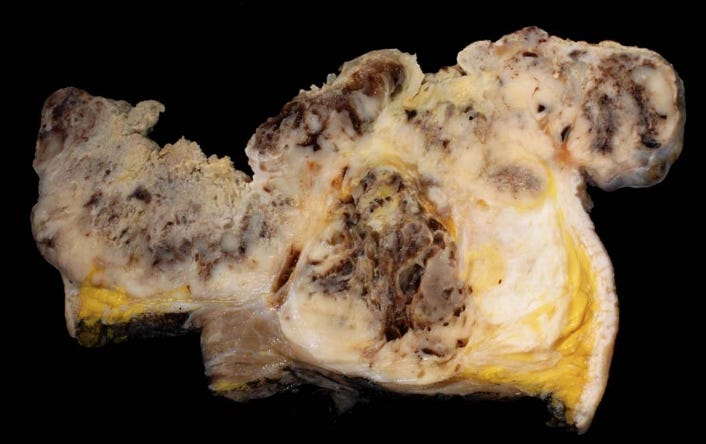
Metaplastic carcinoma, first described in 1973, is a group of invasive breast carcinomas characterized by differentiation towards squamous or mesenchymal cells (spindle, chondroid or osseous). Metaplastic carcinoma is uncommon, representing less than 1% of all breast carcinomas. The mean age of onset is 55 years. It is associated with rapid growth and larger tumors but its clinical presentation is otherwise similar to invasive breast carcinoma of no special type. Grossly, the tumors average 3.9 cm, ranging from 2 to > 10 cm. They are often firm, well circumscribed and solid. They have a pearly white to grayish and glistening cut surface in areas of squamous or chondroid differentiation.
The World Health Organization (WHO) has classified metaplastic carcinoma into six subtypes based on histology (microscopic features): fibromatosis-like metaplastic carcinoma, low grade adenosquamous carcinoma, squamous cell carcinoma, metaplastic carcinoma with heterologous mesenchymal differentiation, spindle cell carcinoma and mixed metaplastic carcinoma.
Fibromatosis-like metaplastic carcinoma and low grade adenosquamous carcinoma are described in detail below.
Squamous cell carcinoma was described previously.
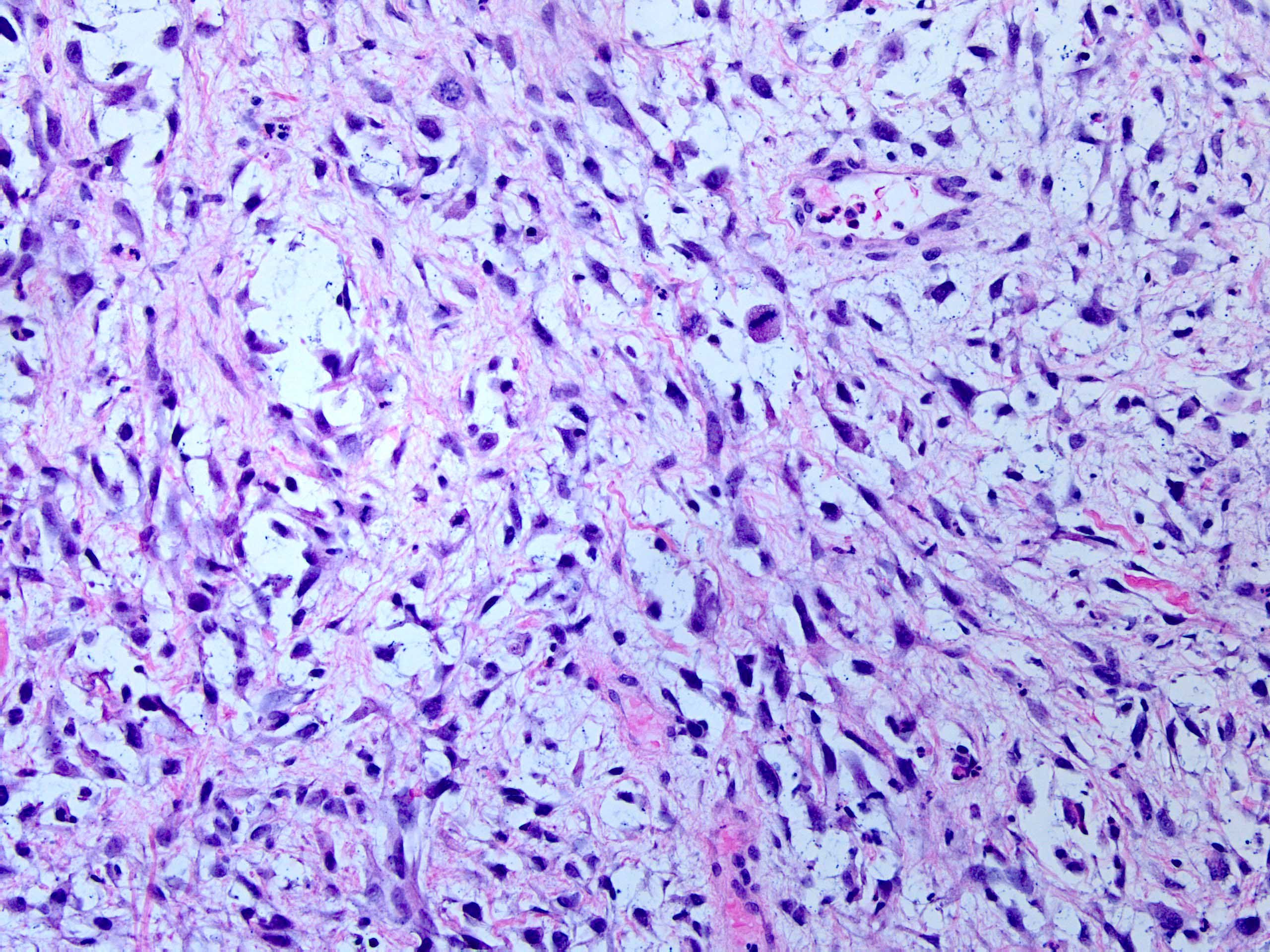
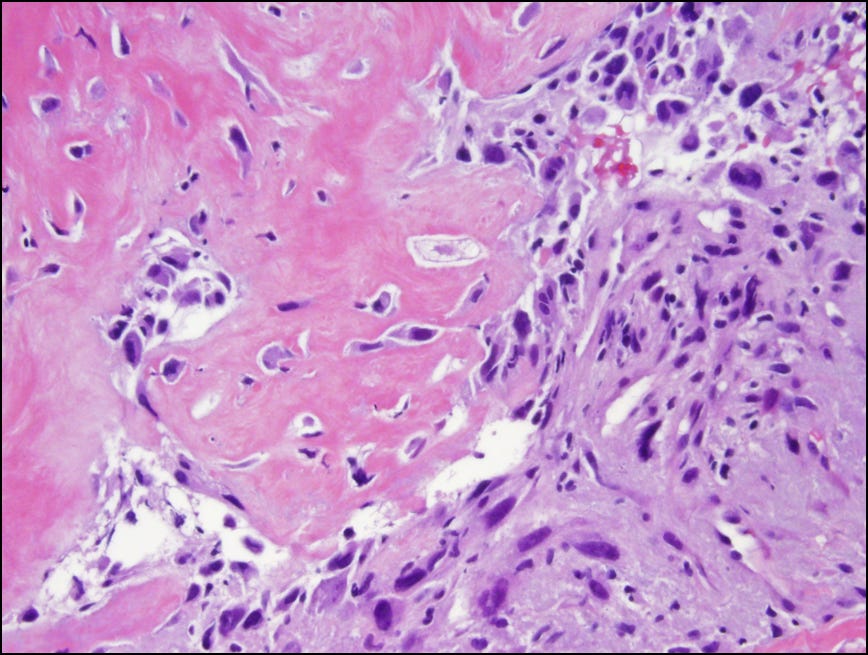
Metaplastic carcinoma with heterologous mesenchymal differentiation has combinations of chondroid, osseous, rhabdomyosarcomatous, angiosarcomatous, liposarcomatous and neuroglial differentiation (heterologous means having a different structure). The mesenchymal component may have atypia ranging from minimal to frankly malignant.
Spindle cell carcinoma has spindle cells resembling those seen in sarcoma, often with atypia, mitotic figures and interspersed collagen fibers.
Mixed metaplastic carcinoma is defined as a tumor with either different metaplastic components or a mixture of metaplastic and conventional adenocarcinoma components.
Pathologists may need to examine the specimen carefully or use cytokeratin immunohistochemical stains to confirm the presence of an epithelial component.
Metaplastic carcinomas are typically triple negative (i.e., negative for ER, PR and HER2). They frequently have mutations in the PIK3CA and TP53 genes.
Treatment is usually mastectomy or local excision, with or without radiation and chemotherapy. There is a poor response to conventional chemotherapy compared to the usual types of breast cancer. Prognosis varies by histologic subtype - high grade spindle cell carcinoma, squamous cell carcinomas and high grade adenosquamous carcinoma have aggressive behavior but fibromatosis-like carcinoma and low grade adenosquamous carcinoma are associated with more indolent behavior.
Metaplastic carcinoma has no known precursor, although it may arise from invasive breast carcinoma of no special type with metaplasia due to transcriptomic (RNA) changes. There is no uniform molecular profile. The mesenchymal component may be monoclonal despite its heterogeneous appearance. It is speculated that the varying histology may be due to epigenetic or noncoding changes.
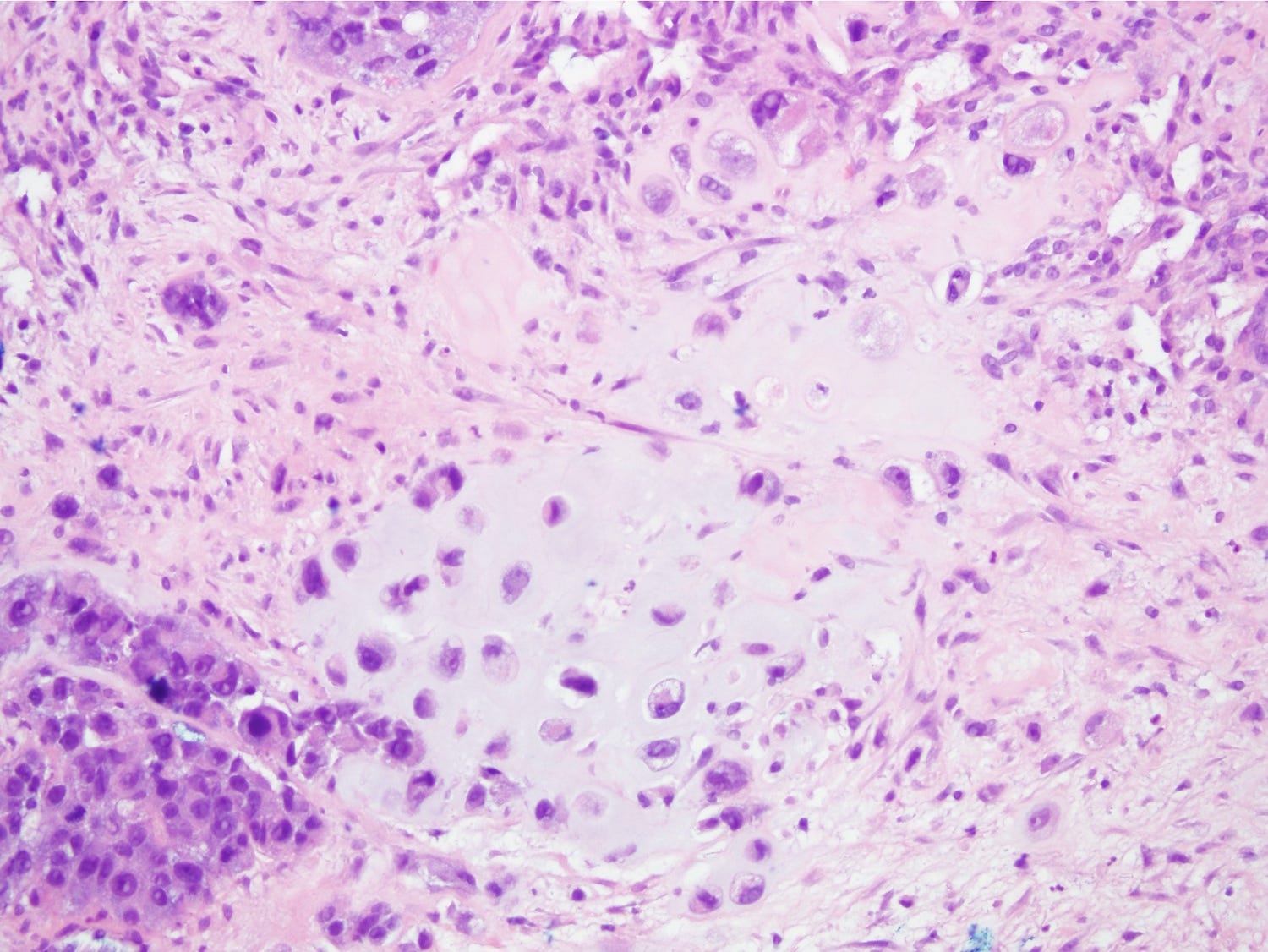
Metaplastic carcinoma of the breast - gross and microscopic images

Fibromatosis-like metaplastic carcinoma of the breast
Fibromatosis-like metaplastic carcinoma is a rare variant of metaplastic carcinoma (< 100 cases reported) that resembles fibromatosis or other benign lesions. Grossly, it is firm, white, typically 2 - 3 cm and nonencapsulated. Microscopically, it is characterized by the proliferation of low grade, spindle shaped, fibroblast-like and myofibroblast-like cells arranged in interlacing fascicles with irregular infiltrative margins into the surrounding breast parenchyma. There is minimal nuclear pleomorphism and no or rare mitotic activity. Immunohistochemical stains (cytokeratins, p63) are needed to establish epithelial differentiation for the diagnosis because in situ and conventional invasive breast carcinoma are usually absent. These tumors are typically triple negative (i.e., negative for ER, PR and HER2). Molecularly, they show genomic stability and no TP53 mutations but do have activating mutations in the PI3K pathway and TERT mutations.
Fibromatosis-like metaplastic carcinoma has a favorable prognosis compared to other metaplastic carcinoma variants. It has a high propensity for local recurrence but lymph node and distant metastases are rare.
Treatment is surgical excision with adequately excised margins. Axillary dissection, chemotherapy and radiation therapy are likely not necessary.
How fibromatosis-like metaplastic carcinoma arises is unknown. It has no known precursor lesions. It may arise de novo (i.e., by itself) or in association with papillary or sclerosing breast lesions.
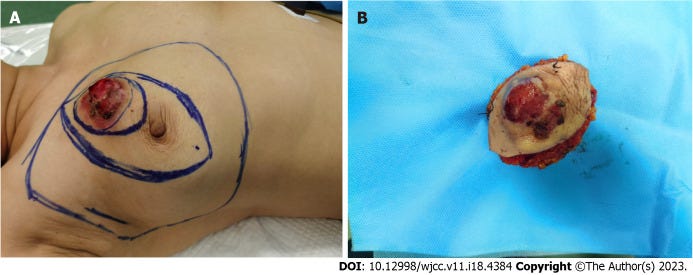
Fibromatosis-like metaplastic carcinoma of the breast - radiologic, clinical, gross and microscopic images







Low grade adenosquamous metaplastic carcinoma of the breast
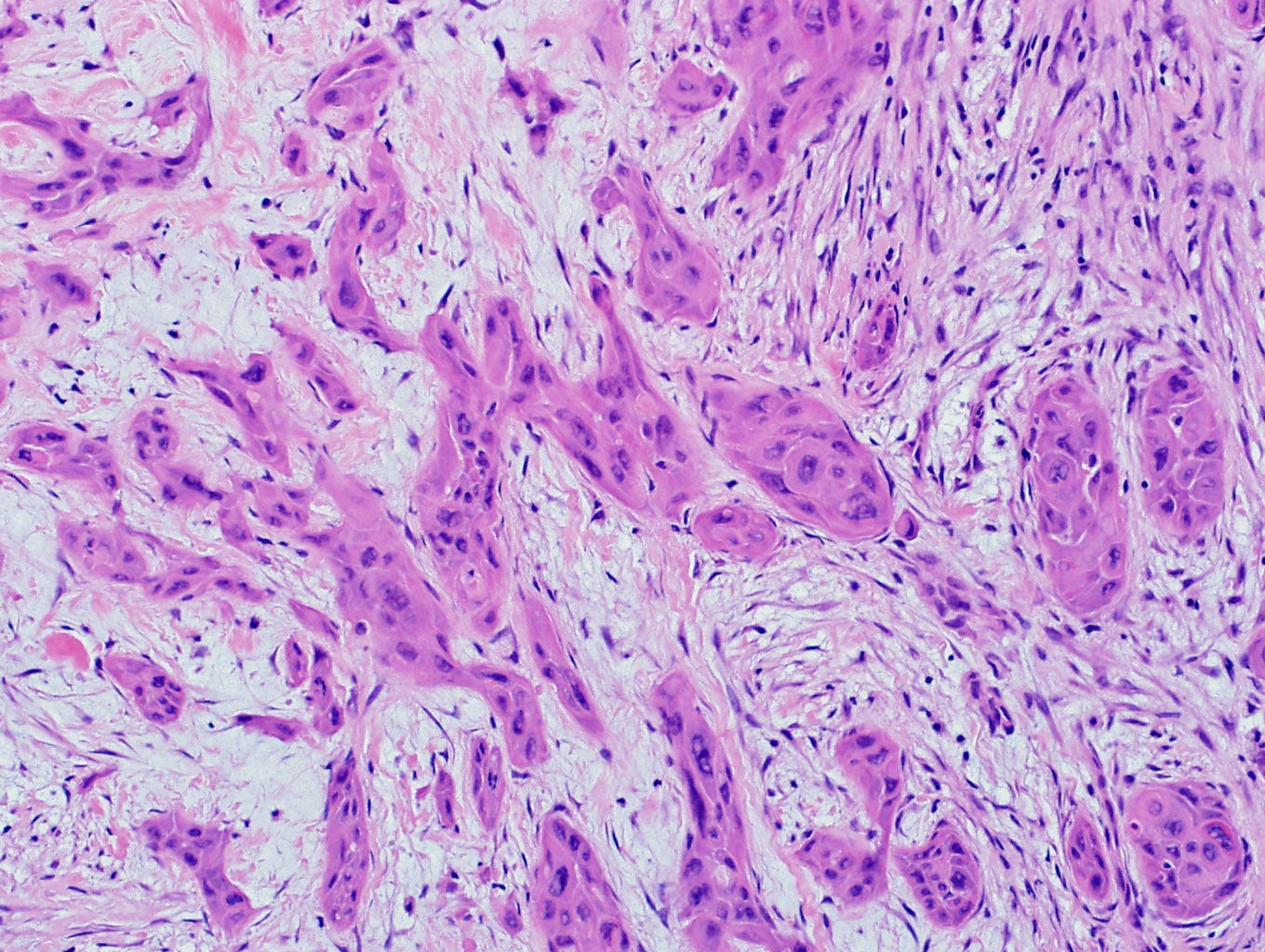
Low grade adenosquamous metaplastic carcinoma is a rare variant of metaplastic carcinoma (0.2 to 1% of all breast carcinomas) composed of both well developed glands and solid squamous cell nests within a fibrotic or cellular spindle stroma. It was first reported in 1917 but only formally recognized in 1987.
Low grade adenosquamous metaplastic carcinoma has relatively bland features, which makes it difficult to diagnose in core biopsies or other small specimens.
The excised specimen is a firm, white or pale yellow tumor, typically less than 5 cm, with ill defined borders. Microscopically, it has infiltrative glandular elements with a variable degree of squamous differentiation. The glands are lined by cytologically bland epithelial cells and may be angulated, compressed or ovoid. Keratin may be present in the lumen. The surrounding stroma may be fibrotic or cellular. Mitotic figures are rare. It is often associated with benign lesions, such as intraductal papilloma, adenomyoepithelioma, radial / complex sclerosing lesions, collagenous spherulosis and fibroepithelial tumors.
It is typically triple negative (i.e., negative for ER, PR, HER2), similar to other metaplastic carcinomas. Molecularly, it often has PIK3CA mutations, found in other metaplastic carcinomas, but lacks TP53 mutations.
Treatment is surgical excision with negative margins. Radiation is indicated for lumpectomies. Whether chemotherapy is beneficial is unclear. It typically has a good prognosis with only rare recurrences after excision in recent studies.
How low grade adenosquamous metaplastic carcinoma arises is unknown although it is associated with proliferative and sclerosing breast lesions. It may arise from adenosquamous proliferation in these lesions, which have a similar histological and immunohistochemical profile and are clonal. It may occasionally arise from metaplasia triggered by retained fragments of localization wires.
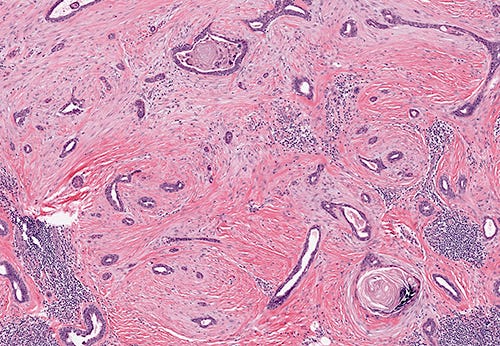
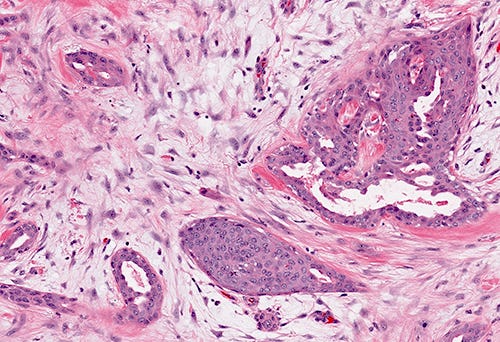
Low grade adenosquamous metaplastic carcinoma of the breast - gross and microscopic images



The next essay, part 6k, will discuss triple negative breast cancers, in general.
If you like these essays, please subscribe or share them with others.
Click here for the Index to Nat’s blog on Cancer and Medicine.
Follow me at https://www.linkedin.com/in/nat-pernick-8967765/ (LinkedIn), npernickmich (Threads and Instagram), natpernick.bsky.social (Bluesky) or @nat385440b (Tribel).
Follow our Curing Cancer Network through our Curing Cancer Newsletter, on LinkedIn or i the CCN section of our PathologyOutlines.com blog. Each week we post interesting cancer related images of malignancies with diagnoses plus articles of interest. Please also read our CCN essays.
Latest versions of our cancer related documents:
American Code Against Cancer (how you can prevent cancer)
Email me at Nat@PathologyOutlines.com - Unfortunately, I cannot provide medical advice.
I also publish Notes at https://substack.com/note. Subscribers will automatically see my Notes.