


Plasma cell myeloma, an overview
4 September 2023

Representative Steve Scalise, the House majority leader, recently announced that he was diagnosed with multiple myeloma (plasma cell myeloma). This overview discusses the disease in general, not his specific case.
General
Myeloid refers both to having a general bone marrow origin as well as to cells with a specific bone marrow lineage that includes neutrophils, basophils, eosinophils, monocytes and macrophages, but NOT lymphocytes.
Plasma cell myeloma is a type of cancer that originates in the bone marrow, but it is a malignancy of plasma cells, which derive from lymphocytes and not myeloid cells; thus the term “myeloma” may be confusing.
Plasma cells produce antibodies, which are composed of immunoglobulins, a type of protein. Each plasma cell produces different antibodies, which maximizes the probability that a person will produce several antibodies that will be effective against any particular microorganism or parasite.
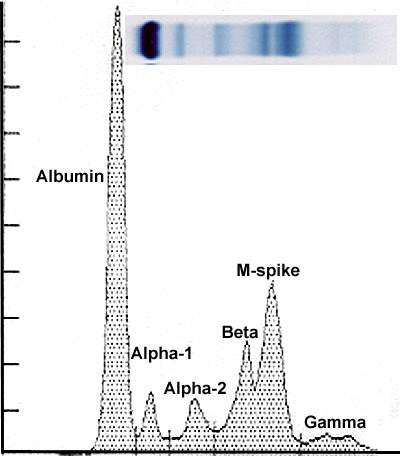
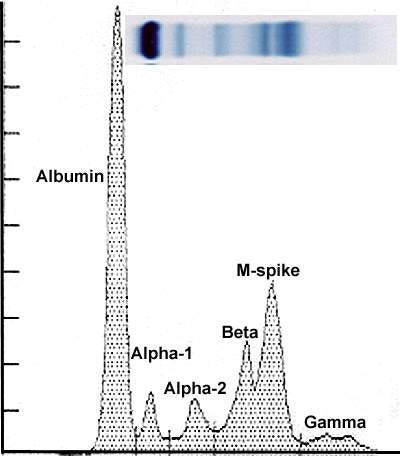
M spike demonstrates the presence of monoclonal plasma cells In plasma cell myeloma, one plasma cell starts the malignant process and produces a large number of malignant plasma cells that all create the same antibody or immunoglobulin. This is identified as a monoclonal or M spike with a blood or urine test called protein electrophoresis.
Epidemiology (who gets it)
Almost all plasma cell myeloma cases arise in patients with a prior diagnosis of monoclonal gammopathy of undetermined significance (MGUS).
MGUS is the diagnosis for patients without evidence of related organ damage.
It is a premalignant condition with an annual risk of progression to plasma cell myeloma of ~1%.
Most plasma cell myeloma patients have no behavioral risk factors.
There is a 2x increased risk in African Americans vs. Whites and for those with an affected first degree relative.
The median age at diagnosis is 70 years.
How plasma cell myeloma arises from benign plasma cells is not known.
Clinical features
Plasma cell myeloma is a type of cancer that is typically multifocal (i.e. occurs at multiple sites).
It is usually associated with a monoclonal immunoglobulin in the serum or urine and evidence of related organ damage.


Lytic bone lesions in the skull, courtesy of Dr. Mark WIck and the Armed Forces Institute of Pathology It frequently includes bone disease, which often presents with bone pain due to lytic bone lesions (i.e. areas where the bone has been destroyed, leaving a hole) in the thoracic vertebrae, ribs, skull, shoulders, pelvis and long bones.
Plasma cell myeloma is often associated with focal or systemic amyloidosis.
Other clinical features are listed here.


Gross (visible with the naked eye) images

The bone lesions are filled with soft, gelatinous "fish flesh", hemorrhagic tissue.
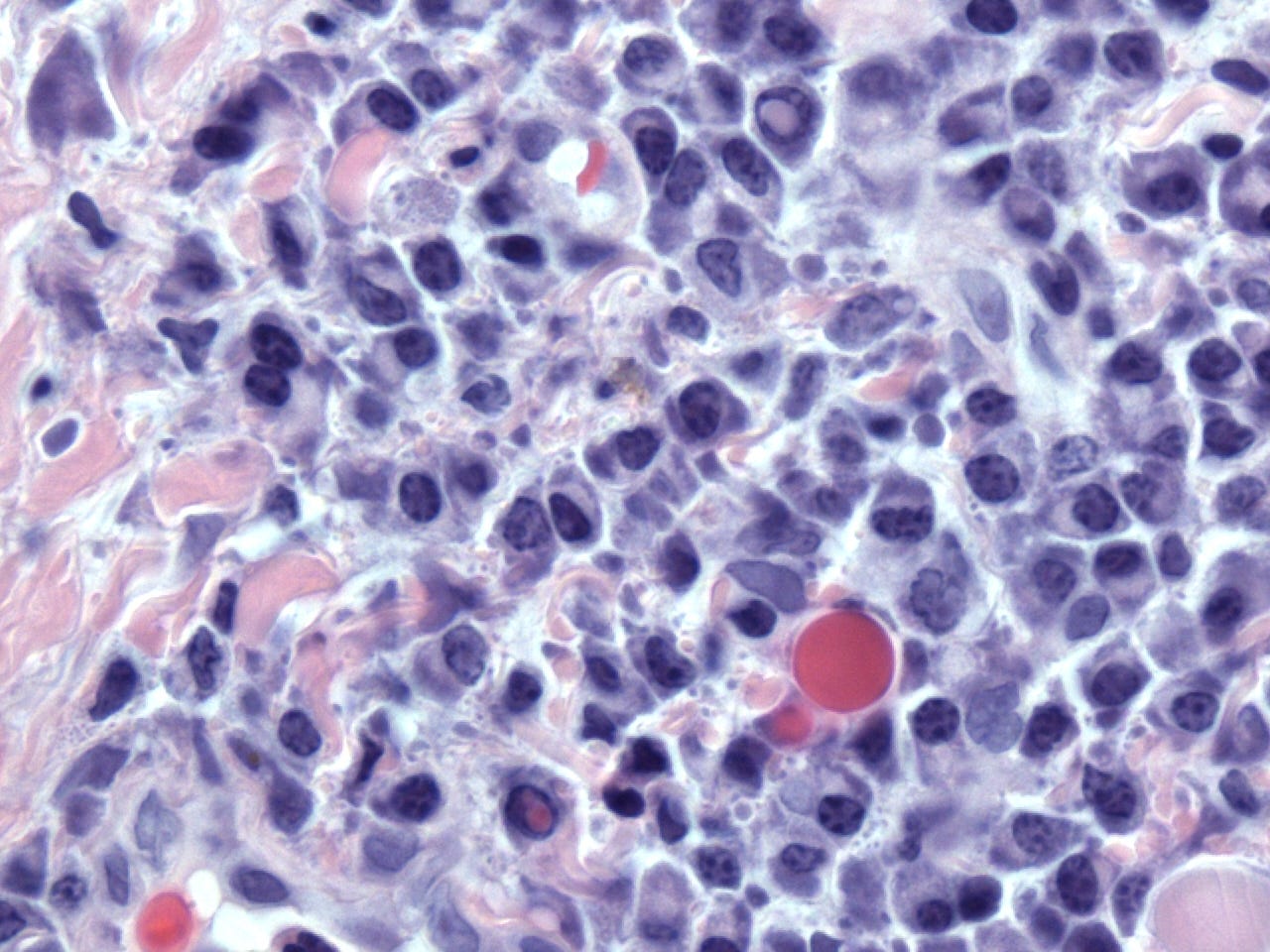
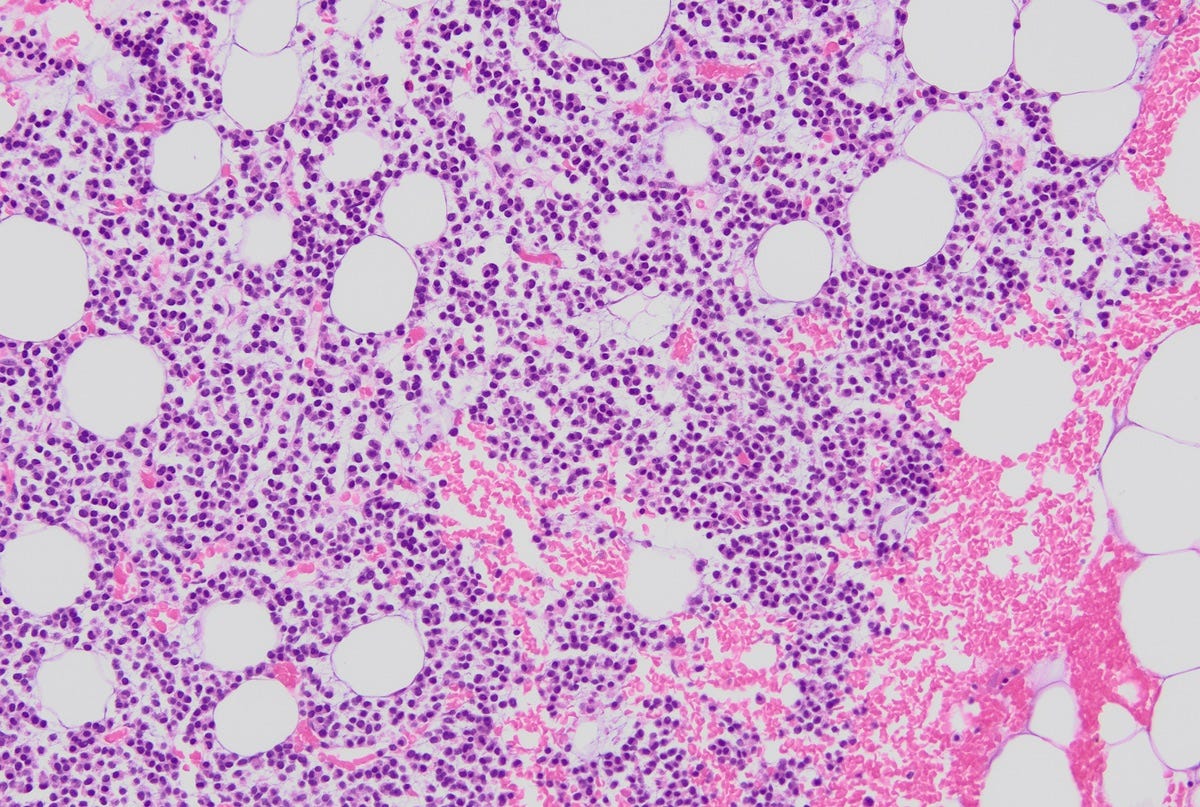
Microscopic images
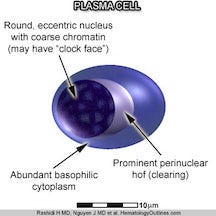
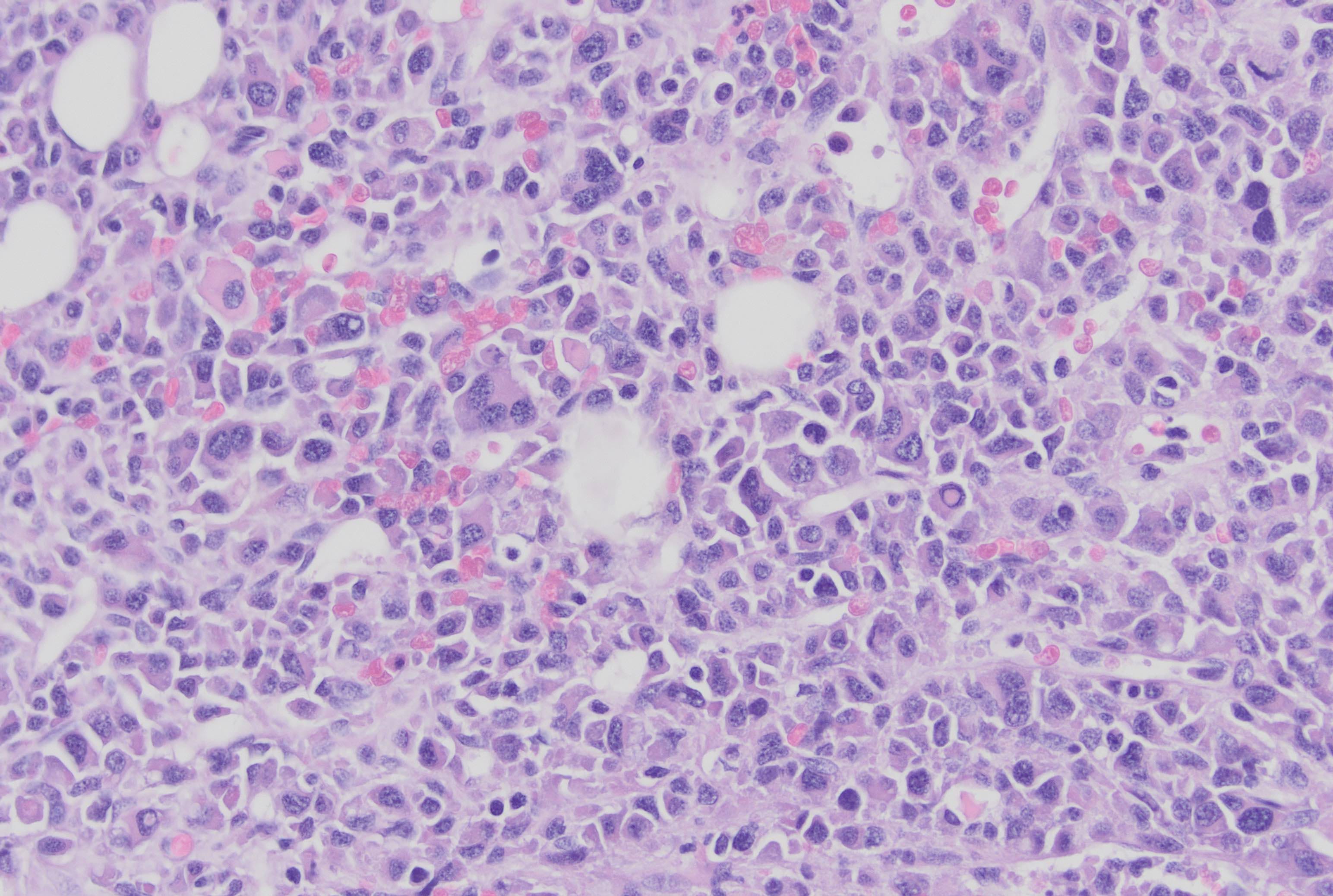
Lesions show a proliferation of plasma cells, which are typically oval with abundant basophilic (blue) cytoplasm, a perinuclear hof (clearing), round eccentric nuclei, clock face chromatin and indistinct nucleoli.
Atypical plasma cells may be present, with a higher nuclear to cytoplasmic ratio, more abundant cytoplasm, and more prominent hof regions and nucleoli.

Focal sheets of plasma cells 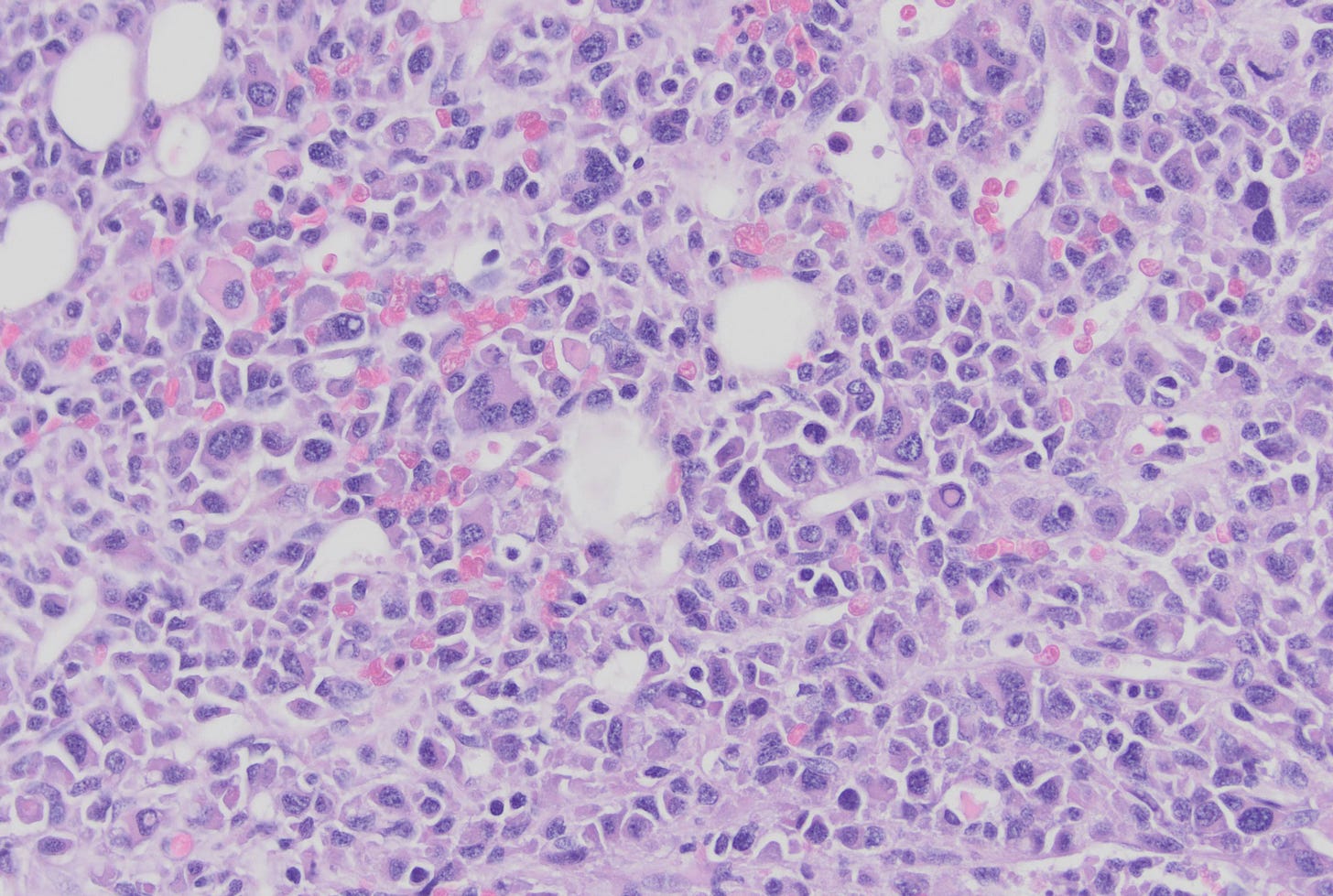
Atypical plasma cells with variable cell sizes, variable nuclear shapes (pleomorphism) and multinucleated forms. 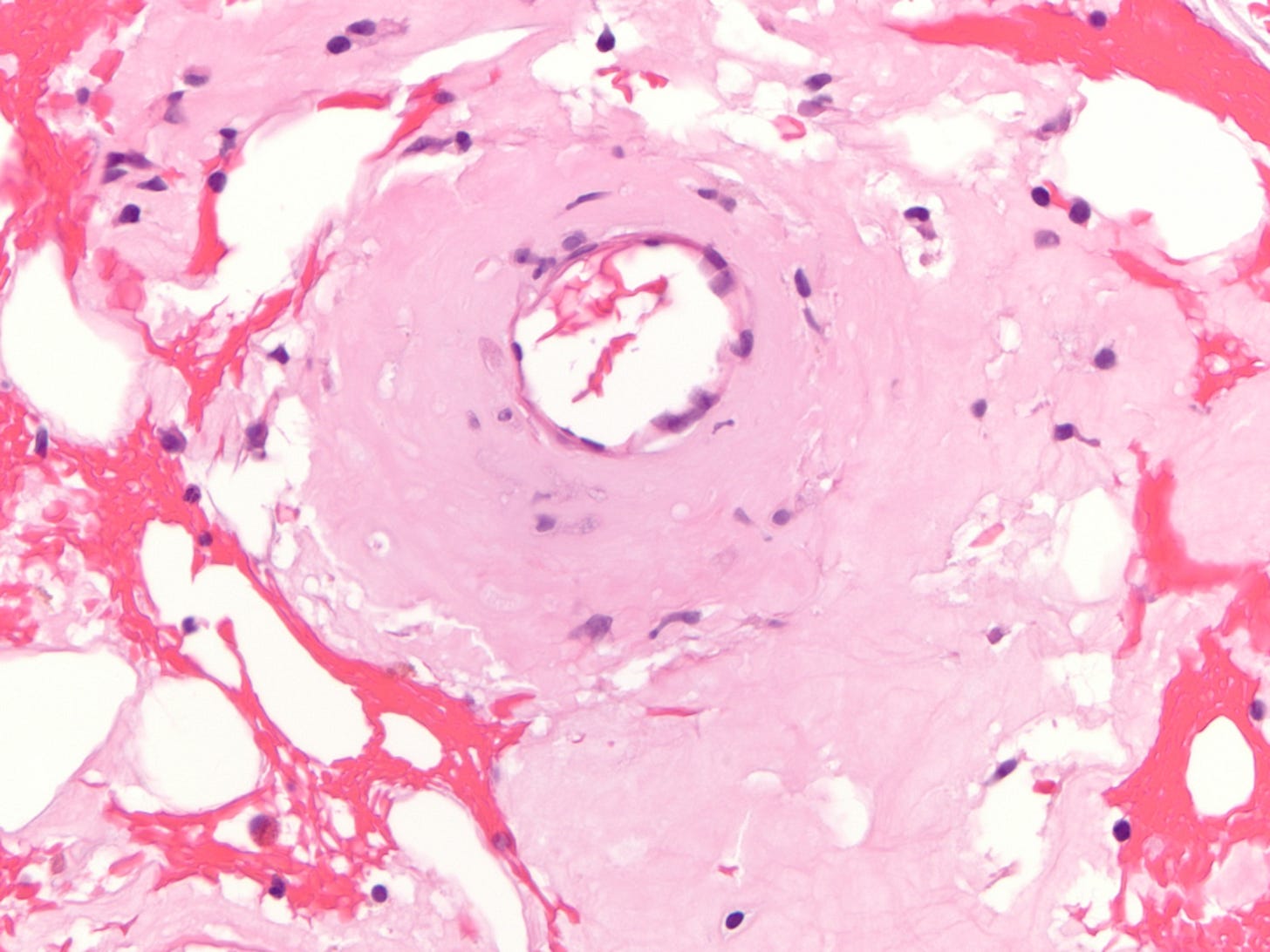
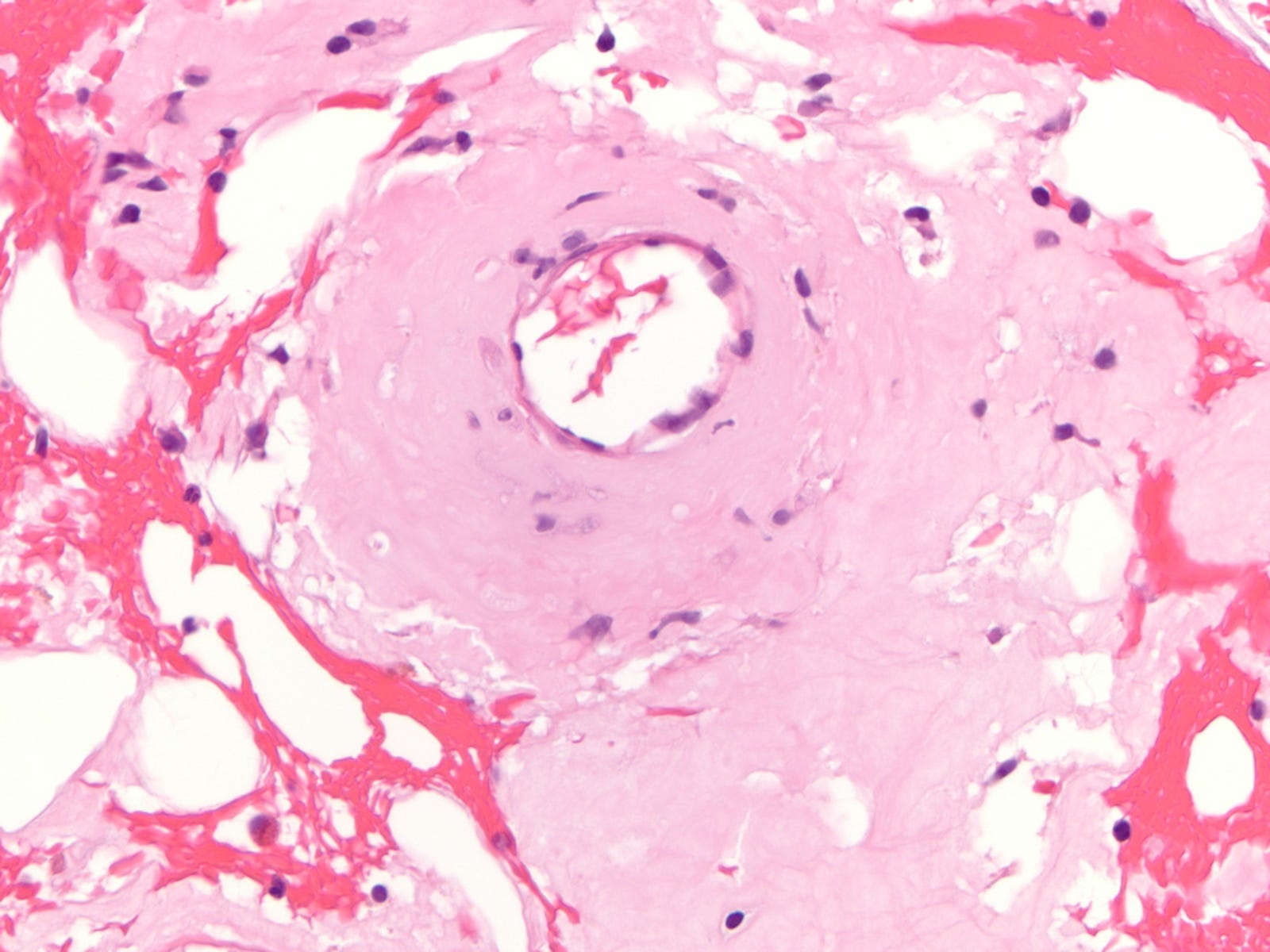
Bone marrow blood vessels showing extensive amorphous material consistent with amyloid Plasma cell myeloma is highly treatable but rarely curable. In the prechemotherapy era, the median survival was 7 months. Today, using chemotherapy and newer biological therapies, the median survival exceeds 10 years.
End of discussion.
Index to Nat’s Substack articles
If you like these essays, please share them with others.
Follow me on Substack or LinkedIn or through our Curing Cancer Newsletter.
Follow our Curing Cancer Network on LinkedIn and Twitter. Each week we post interesting cancer related images of malignancies with diagnoses.
Latest versions of our cancer related documents:
American Code Against Cancer (how you can prevent cancer)
Email me at Nat@PathologyOutlines.com - Unfortunately, I cannot provide medical advice.
I also publish Notes at https://substack.com/note. Subscribers will automatically see my notes.
Other social media - Tribel: @nat385440b, Instagram / Threads: npernickmich