


Cancer precursor project - breast cancer, part 6c
17 December 2024, updated 4 February 2024

In part 6a, we discussed breast cancer mortality, breast cancer risk factors and how breast cancer arises. In part 6b, we discussed breast anatomy and histology and three breast cancers with known precursors: infiltrating duct carcinoma of no special type, lobular carcinoma and pleomorphic lobular carcinoma. We also discussed their precursors of ductal carcinoma in situ (DCIS), classic lobular carcinoma in situ (LCIS) and its variants florid and pleomorphic LCIS, and atypical lobular hyperplasia. In this essay (part 6c), we discuss 4 other types of breast carcinoma with ductal carcinoma in situ (DCIS) as a precursor: cribriform carcinoma, secretory carcinoma, neuroendocrine-small cell carcinoma and male invasive breast carcinoma.
Cribriform carcinoma of the breast
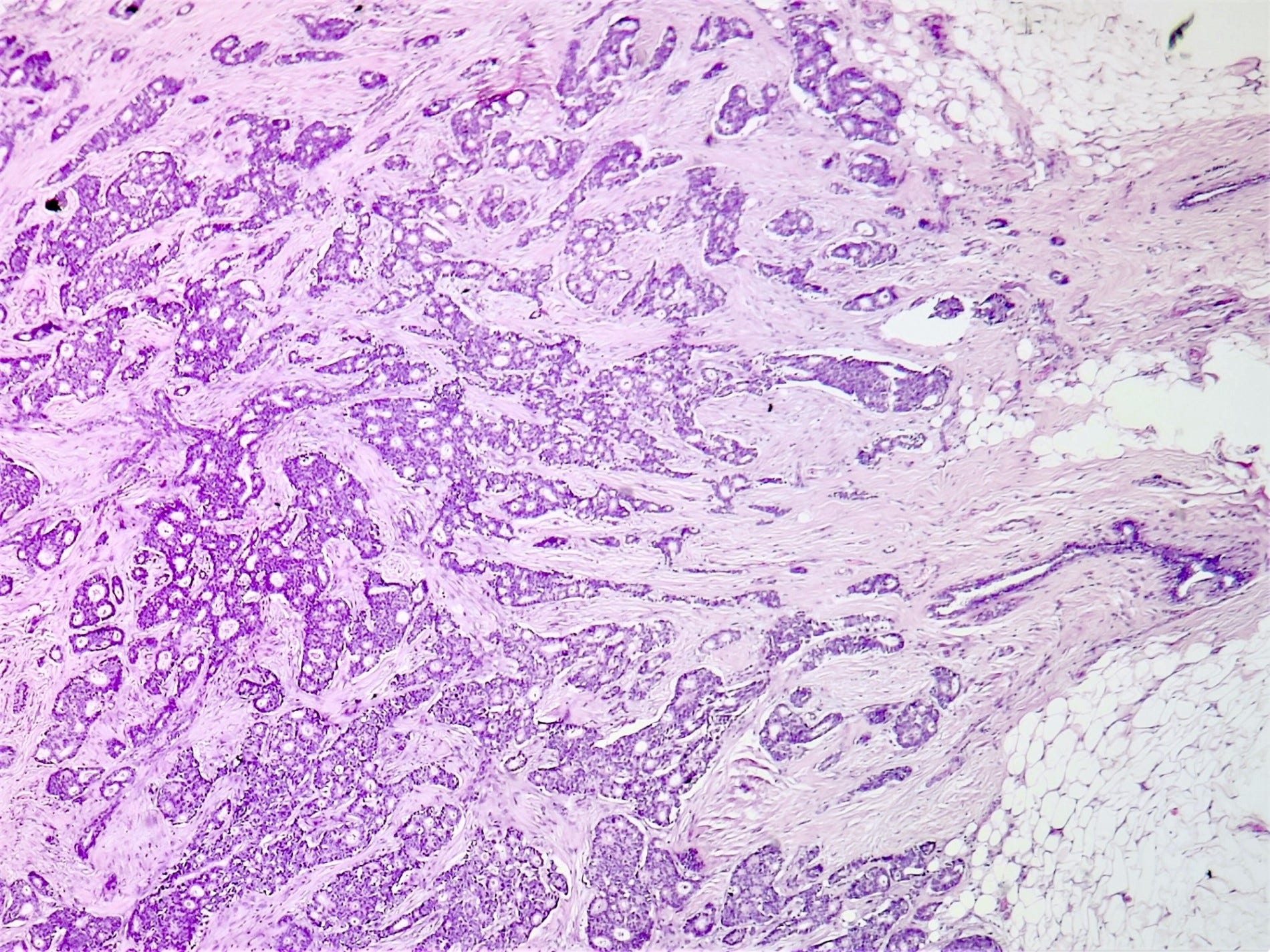
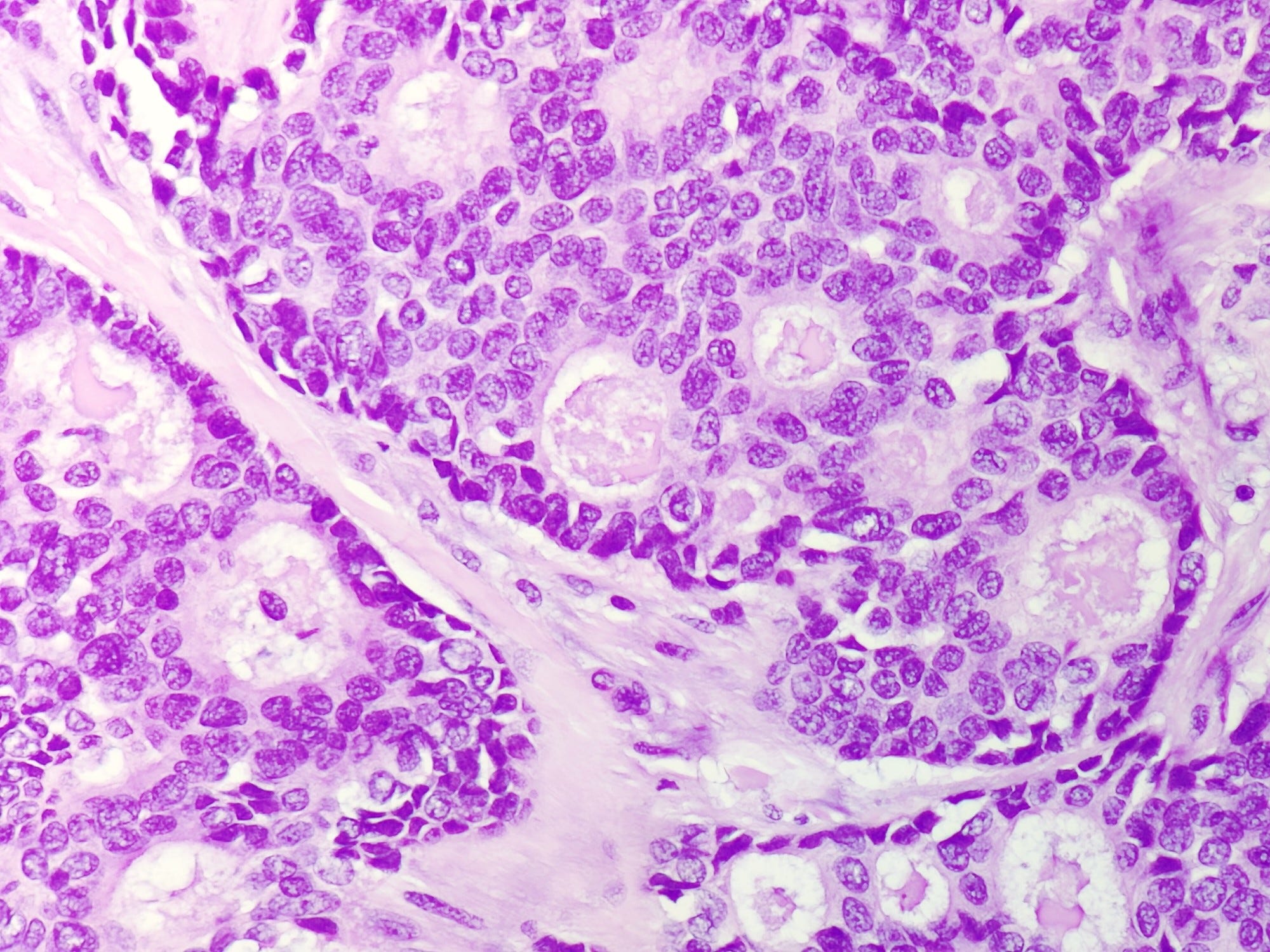
Cribriform carcinoma of the breast is a rare (0.3 - 3.5% of breast carcinomas), low grade (i.e. relatively nonaggressive) invasive breast carcinoma characterized by a predominant cribriform (sieve-like or Swiss cheese) microscopic pattern of malignant epithelial cells. It may be pure (cribriform architecture comprises > 90% of the tumor) or mixed (tumor is composed of 10 - 90% of another morphological type). It typically expresses estrogen and progesterone receptors (ER / PR) but lacks HER2 overexpression.
It may present as a small lump or be asymptomatic and is multifocal in 10 - 20% of cases. Lymph node metastases are present in 14% of pure cases and 25% of mixed cases.
Treatment consists of surgery, endocrine therapy and possibly radiation therapy. Prognosis is excellent for pure cases. It is poorer for mixed cases but still more favorable than invasive ductal carcinoma of no special type.
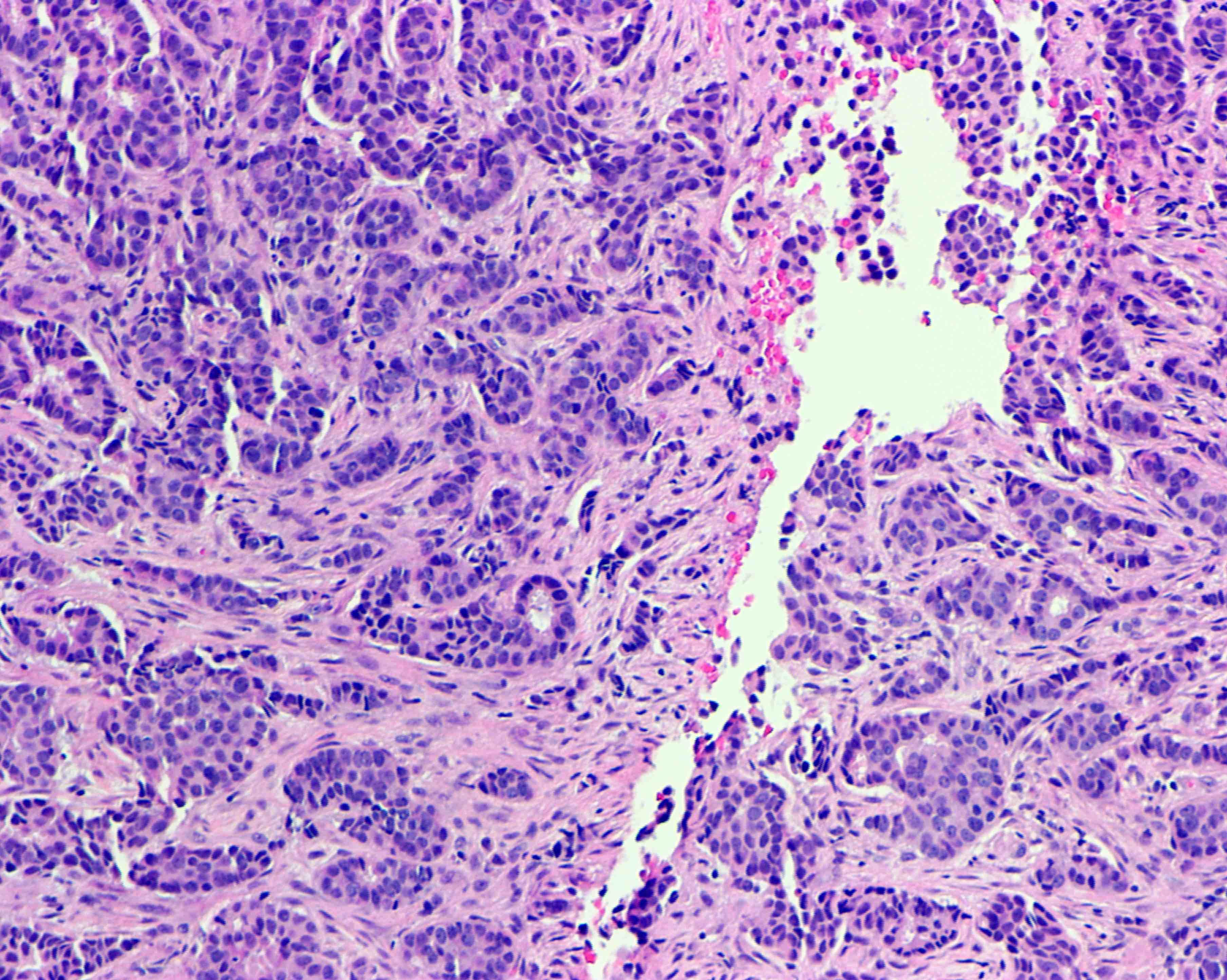
The excised specimen is usually small (< 2 cm) with a firm or hard spiculated mass (having points on its surface) and is gritty if calcifications are present. Microscopically, there are invasive islands or nests of malignant cells with round or angulated contours and well defined cribriform spaces formed by arches of epithelial cells; this gives a sieve-like appearance. The malignant cells are small, with mild to moderate pleomorphism and no nuclear atypia. There is no or sparse mitotic activity and the stroma is desmoplastic (fibrous). These tumors are often associated with cribriform DCIS, which may be a precursor.
The cribriform pattern, although not present in normal breast epithelium, is present in many breast lesions including two benign lesions: collagenous spherulosis and atypical ductal hyperplasia and two malignancies: adenoid cystic carcinoma and well differentiated neuroendocrine tumor.
In the prostate, the cribriform pattern is seen in normal prostate epithelium from the central zone, benign lesions of clear cell cribriform hyperplasia and basal cell hyperplasia, premalignant lesions of high grade prostatic intraepithelial neoplasia and atypical intraductal proliferation and malignant lesions of intraductal, acinar, ductal and basal cell carcinoma.
The cribriform pattern may be due to the mechanical piling up of cells within a preexisting duct. In malignant lesions, it may be due to “a constellation of unfavorable molecular characteristics.” Whether this analysis applies also to cribriform lesions in the breast is unclear.
Cribriform patterns also occur in these lesions: adenoid cystic carcinoma at various sites), cervix-HPV associated carcinoma, colon-adenomas, colon-cribriform carcinoma, lung-enteric adenocarcinoma, ovary-serous borderline tumor, salivary gland-intraductal carcinoma, salivary gland-polymorphous adenocarcinoma, thyroid-cribriform-morular carcinoma, uterus-endometrioid carcinoma and occasionally in other lesions.
The transformation of DCIS, including cribriform DCIS, into invasive breast cancer may involve changes to the myoepithelial cells surrounding breast epithelium through tissue mechanical changes and cell signaling pathways.
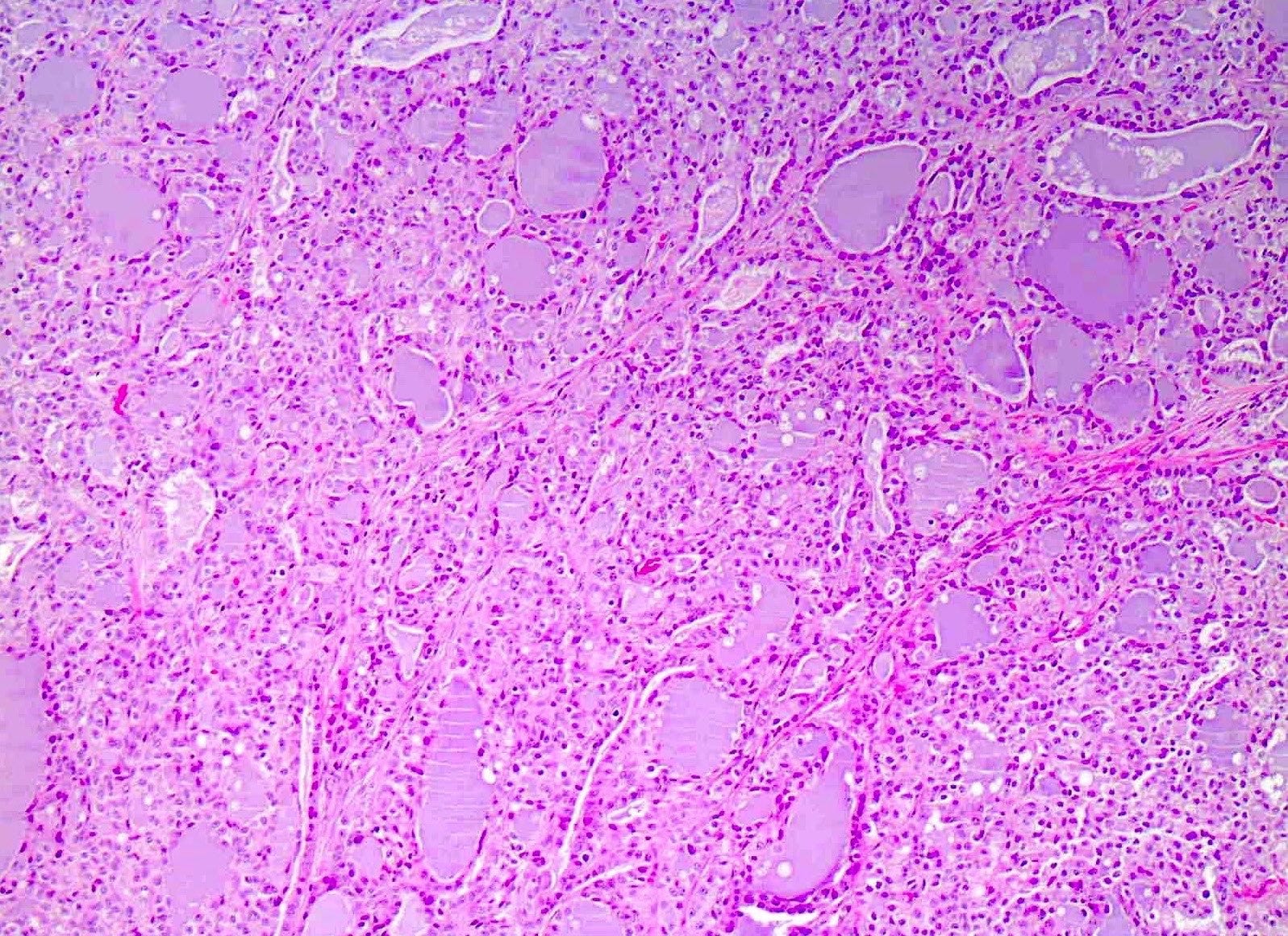
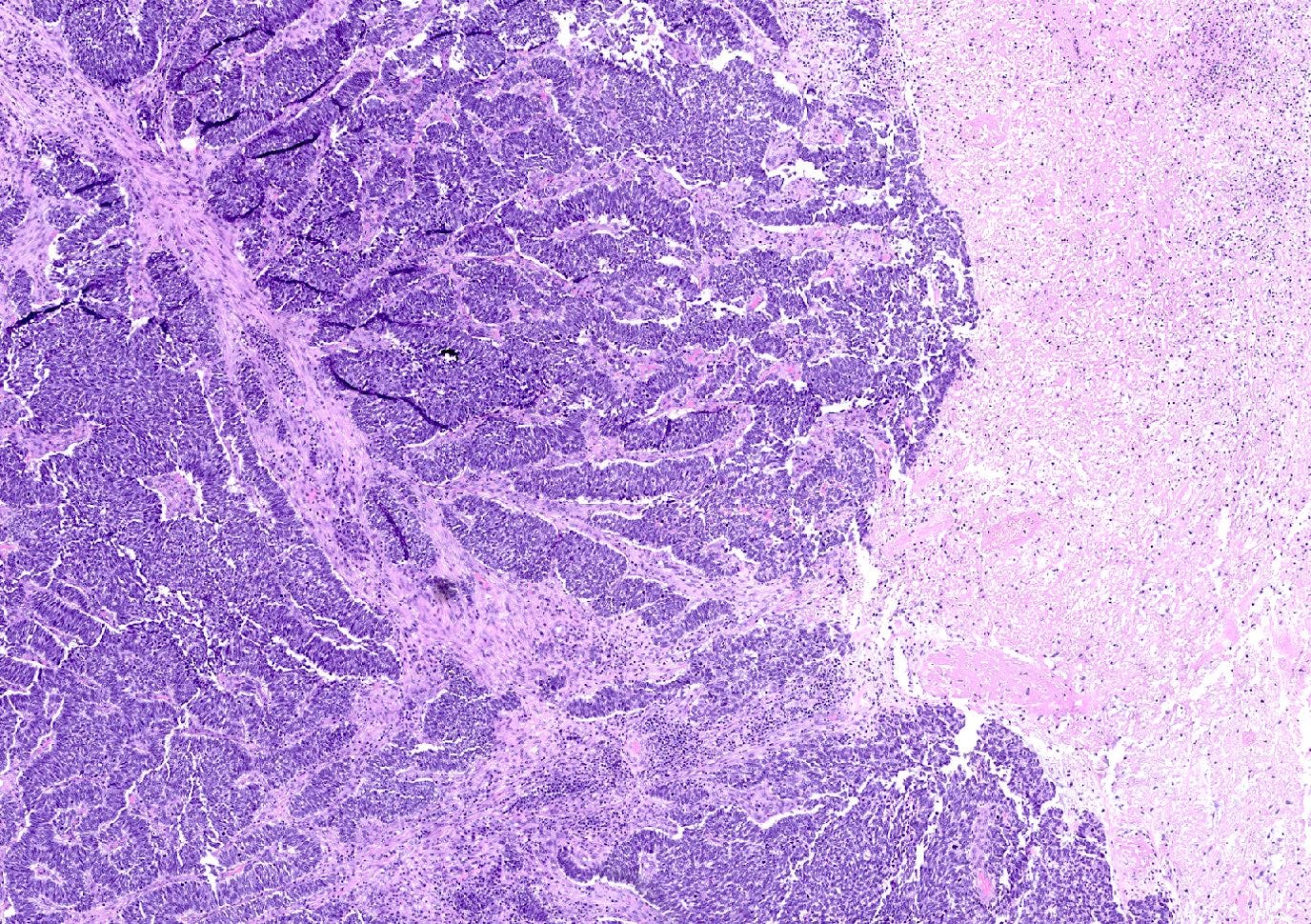
Cribriform carcinoma - microscopic images
Secretory carcinoma of the breast
Secretory carcinoma of the breast is a rare (< 0.2 % of breast cancers), low grade, invasive breast carcinoma first described in 1966. It has an excellent prognosis with a 5 year overall survival of 87% and a 5 year disease specific survival of 94%.
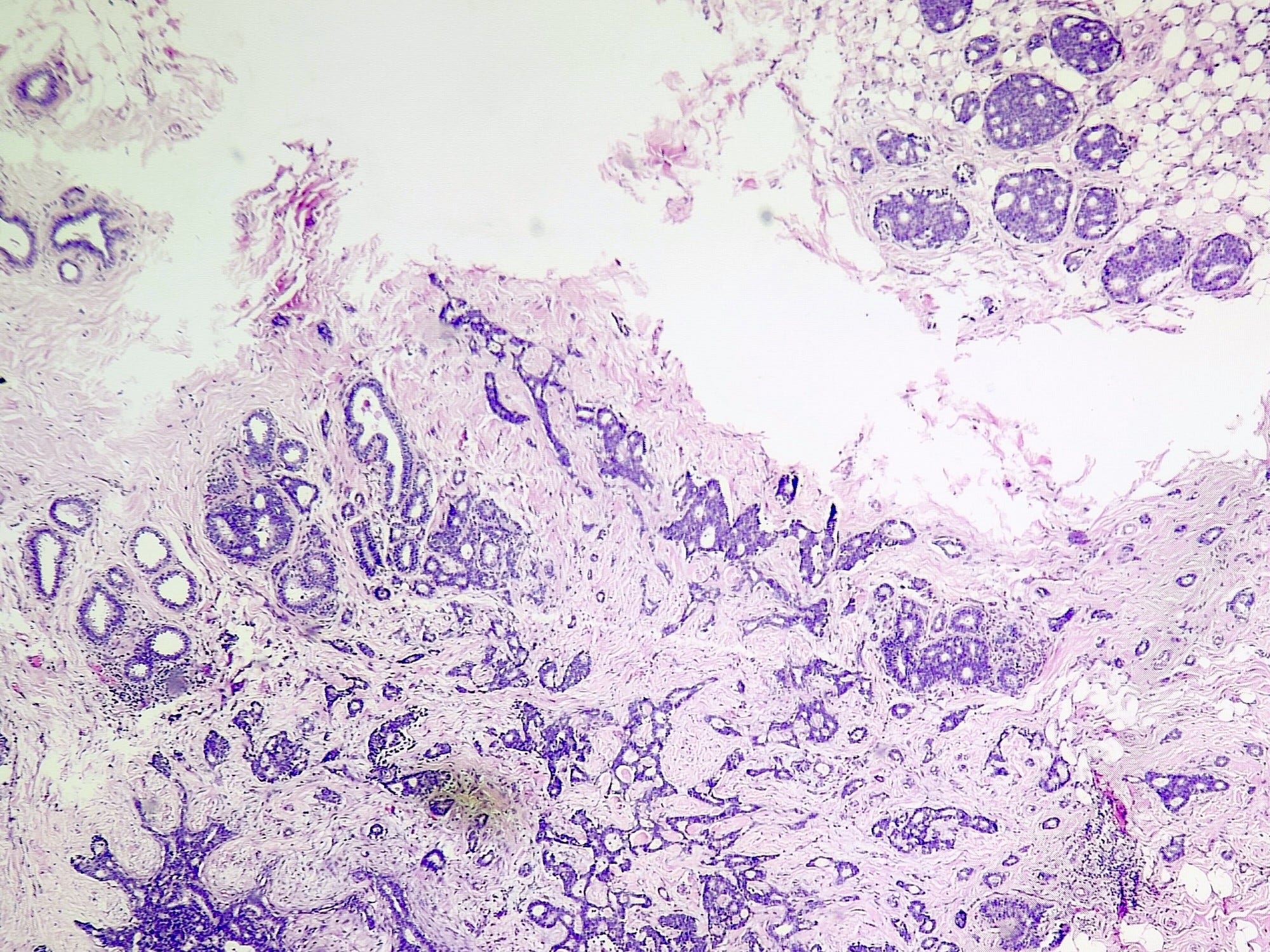
Microscopically, it has a microcystic, solid and tubular architecture and is composed of vacuolated tumor cells producing intracellular and extracellular secretions. It is the most common primary pediatric breast cancer but can occur at any age.
Secretory carcinoma is associated with the chromosomal translocation t(12;15)(p13;q25), resulting in an ETV6-NTRK3 fusion gene in 95% of cases, which produces a protein with transforming properties. Translocations are due to replication errors during cell division, environmental factors or genetic predisposition. These errors cause chromosome breaks in the wrong place, at the wrong time associated with factors that promote the translocation or a delayed repair. The specific factors associated with this translocation are unknown.
The t(12;15)(p13;q25) is also associated with other malignancies including infantile fibrosarcoma, congenital mesoblastic nephroma and rarely acute myeloid leukemia.
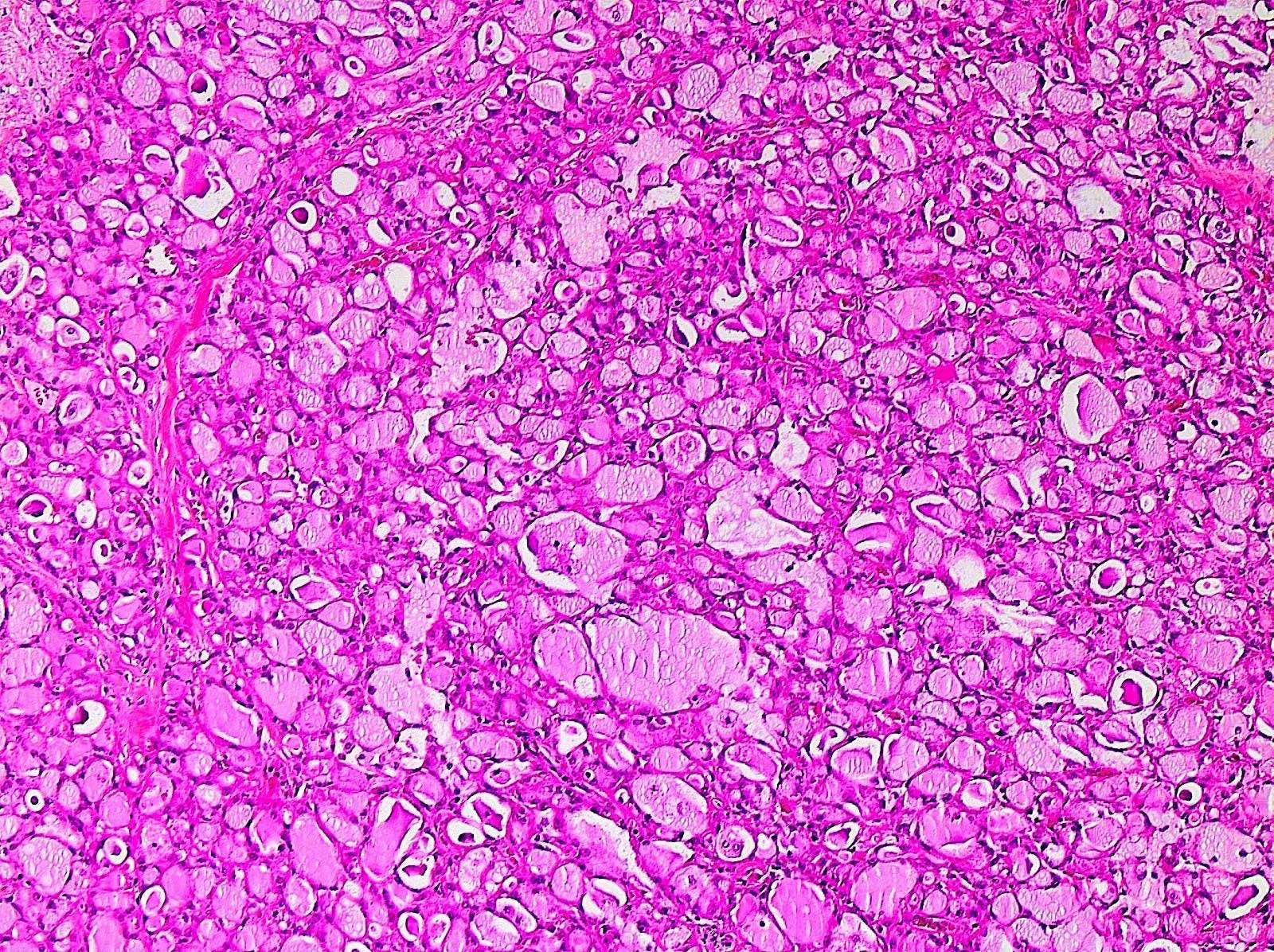
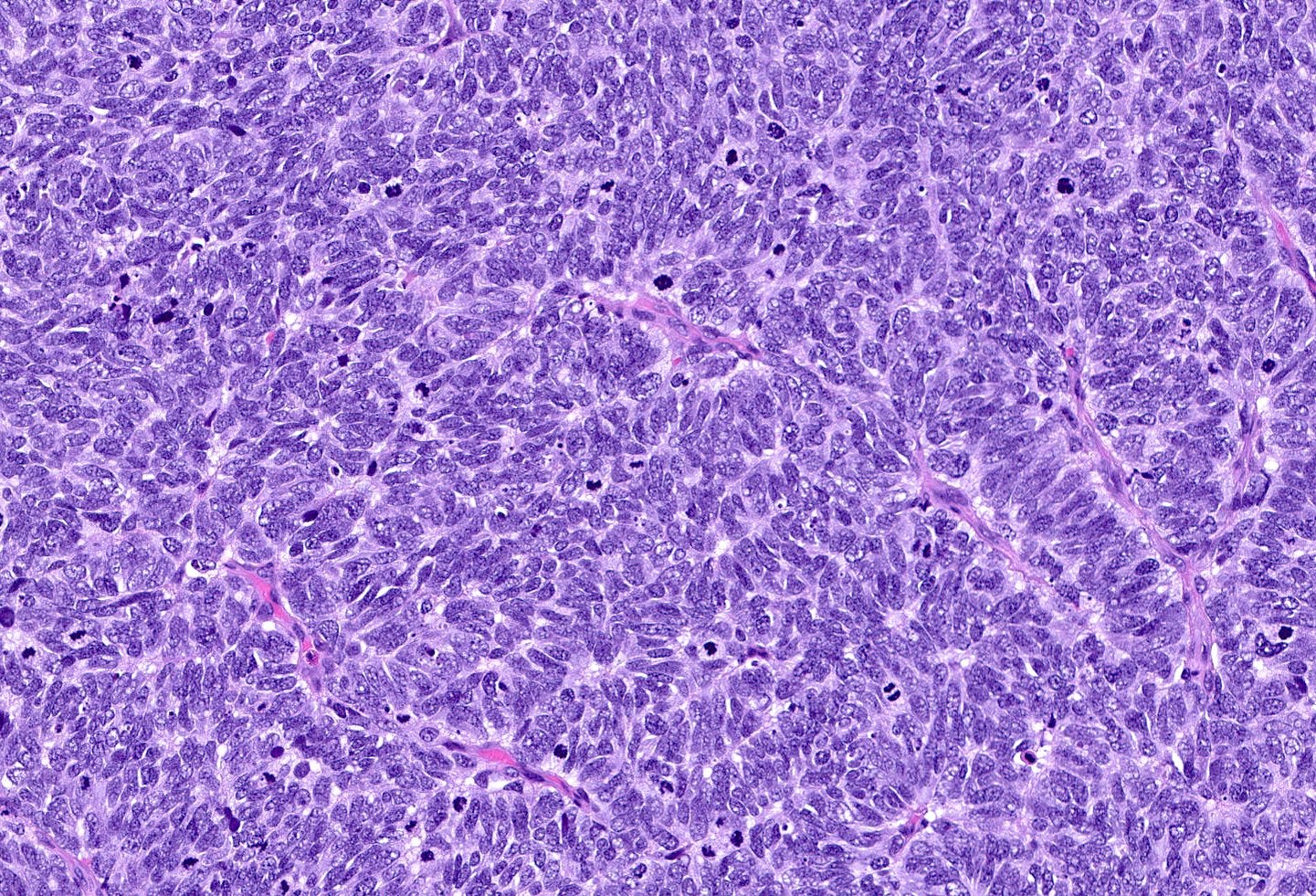
Secretory carcinoma - microscopic images
Neuroendocrine-small cell carcinoma of the breast
Neuroendocrine-small cell carcinoma is a rare (0.1% of primary breast cancers) invasive carcinoma that resembles small cell carcinoma of the lung and other sites and typically affects postmenopausal women. It has high grade (aggressive) neuroendocrine features and is immunoreactive to neuroendocrine markers. It typically presents as a mass lesion 1 - 11 cm, frequently with distant disease (31% versus 5% for breast cancer overall). It is composed of small, dark tumor cells with ill defined borders, scant cytoplasm, hyperchromatic nuclei, inconspicuous nucleoli and frequent mitotic figures. There is often a crush artifact, necrosis and lymphovascular invasion. It is often associated with DCIS, which is considered a precursor lesion.
Neuroendocrine cells receive signals from the central or peripheral nervous system and release hormones as appropriate into the bloodstream.
Small cell carcinoma of the breast is thought to derive from the divergent differentiation of a neoplastic breast epithelial progenitor cell because (a) these cancers are microscopically similar to common breast cancers, (b) all undifferentiated breast cancer cells are considered to possess the ability to express neuroendocrine markers and (c) unlike in the lung, GI tract or prostate, benign neuroendocrine cells have not been reported in the breast.
In the prostate, neuroendocrine differentiation can be induced by IL6 (interleukin 6), Dovitinib, an anti-cancer agent used for myeloma and acute myeloid leukemia, fractionated ionizing radiation, androgen-deprivation therapy (ADT) and therapies affecting the cAMP pathway. However, none of these factors appear to be relevant in the development of small cell carcinoma of the breast.
For diagnosis, it is important to exclude metastases from another site, which requires an adequate history and physical exam. The presence of DCIS suggests that the small cell carcinoma arose in the breast.
Treatment consists of surgical resection, usually with lymph node resection and hormonal therapy. Small cell carcinomas of the breast show worse survival than other breast malignancies but better than small cell carcinoma of the lung.
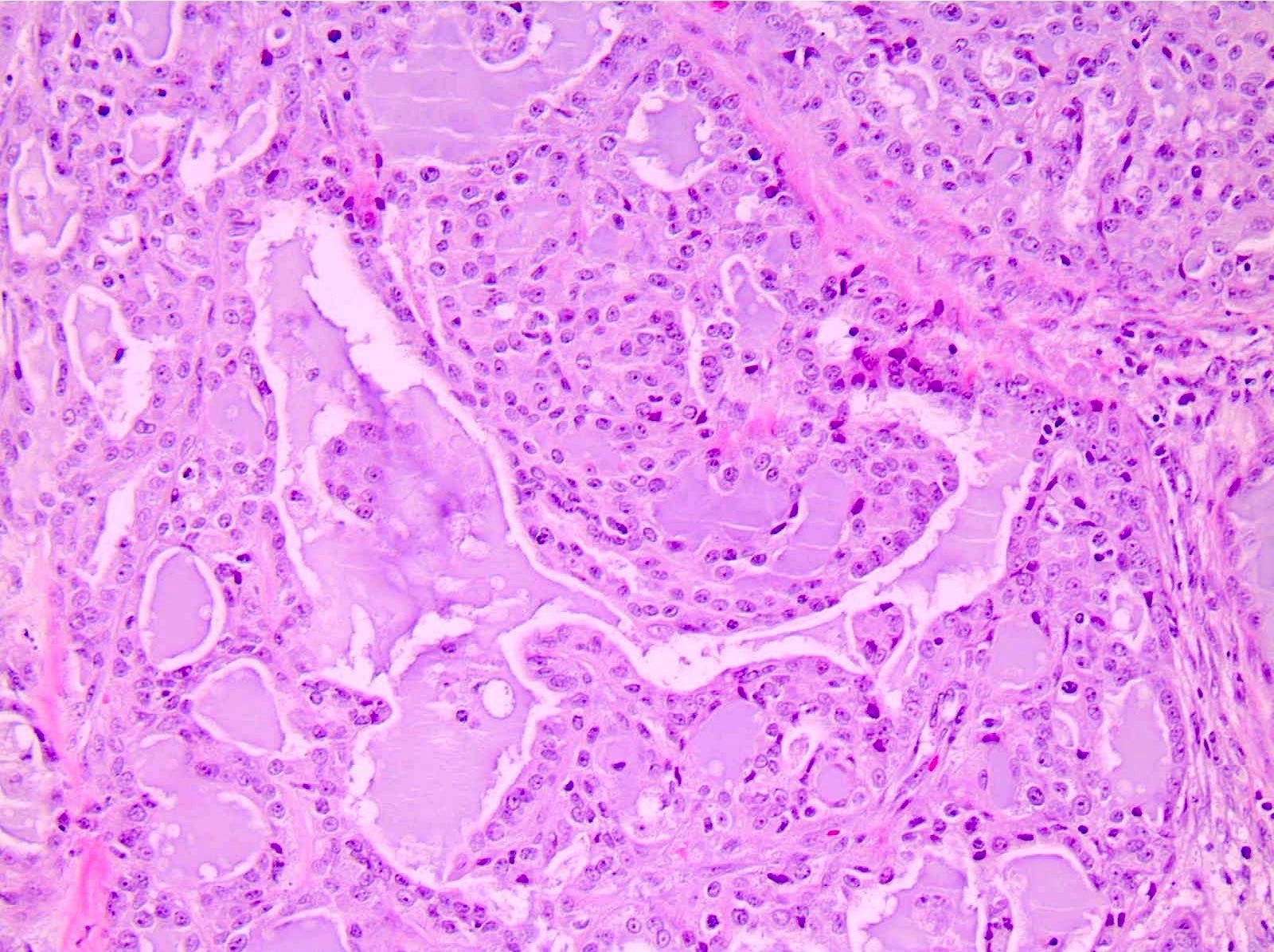
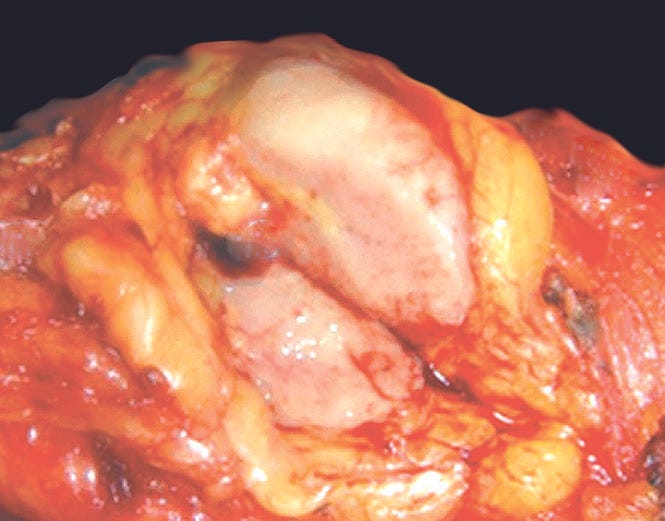
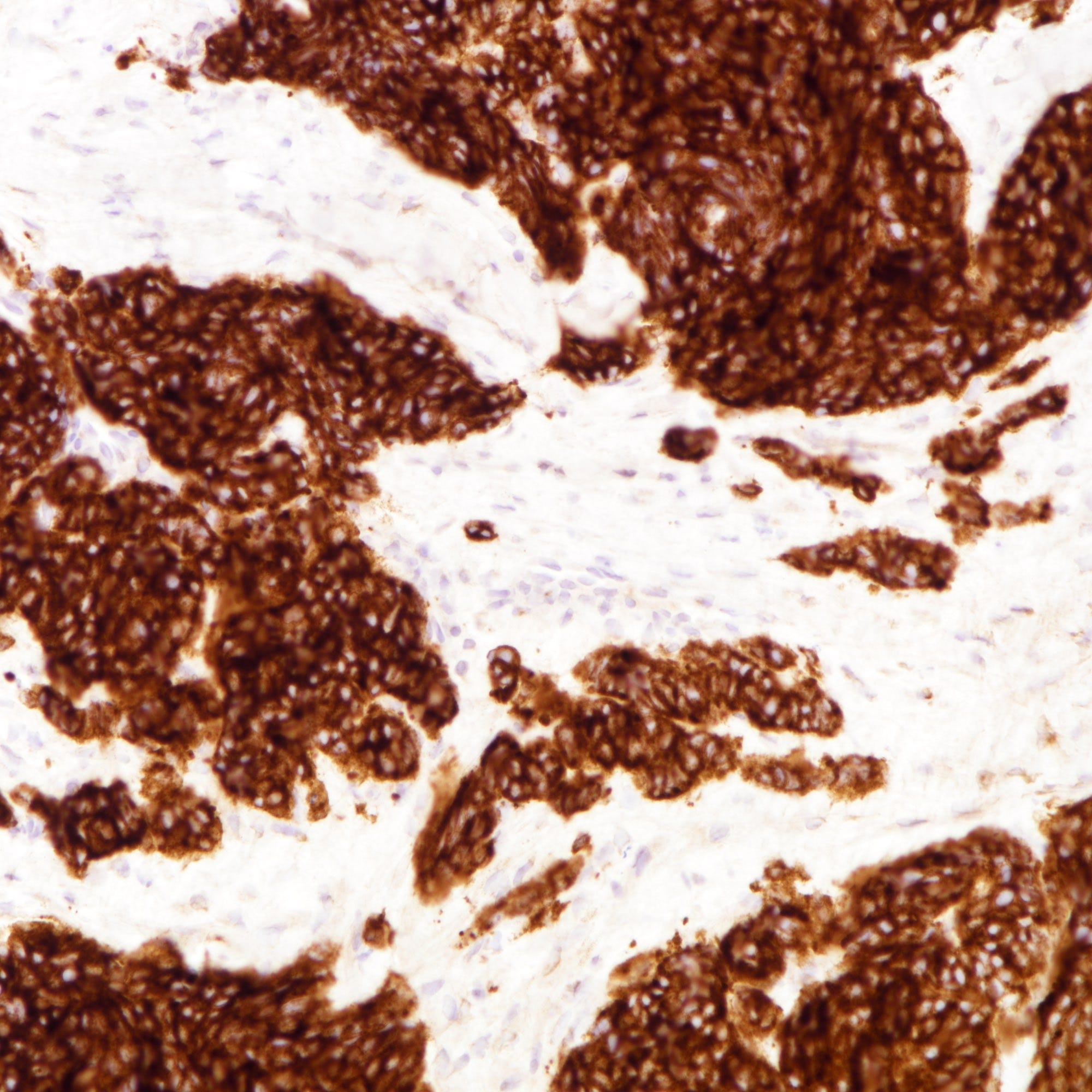
Small cell carcinoma of the breast - gross and microscopic images
Male invasive breast carcinoma
Invasive breast carcinoma in men is rare, accounting for < 1% of all male cancers and 0.1% of male cancer deaths. Invasive breast cancer tends to occur at an older age in men versus women (60 - 70s versus 50 - 60s) and has a larger tumor size. The estimated lifetime risk in BRCA2 carriers is 4% or 40 times the risk of 0.1% in the general male population. Other mutations associated with male breast cancer are PTEN (Cowden syndrome) and CHEK2.
Male breast cancer is associated with (a) increased serum estrogens due to liver disease, obesity, exogenous therapy and antiandrogen therapy; (b) decreased serum androgens due to Klinefelter syndrome, testicular injury or atrophy and occupational exposure to high temperatures; (c) use of digitalis, tricyclic antidepressants, marijuana, lavender oil and tea tree oil; (d) radiation therapy for other cancers and (e) hyperprolactinemia.
Most male breast cancer patients present with a larger mass and at a higher stage than women. They have a 30x increased risk of invasive carcinoma in the other breast, increasing to 110x if the original diagnosis was before age 50. Lymph node metastases are more common in men than women.
Most men are treated with mastectomy and axillary lymph node dissection, based on guidelines for female breast cancer. The death rate is higher among nonwhite men in the United States and lower among Japanese men in Japan.
In a 2019 study, the overall survival rate was 46%, the 3 year rate was 86% and the 5 year rate was 78%, which is much lower than in women.
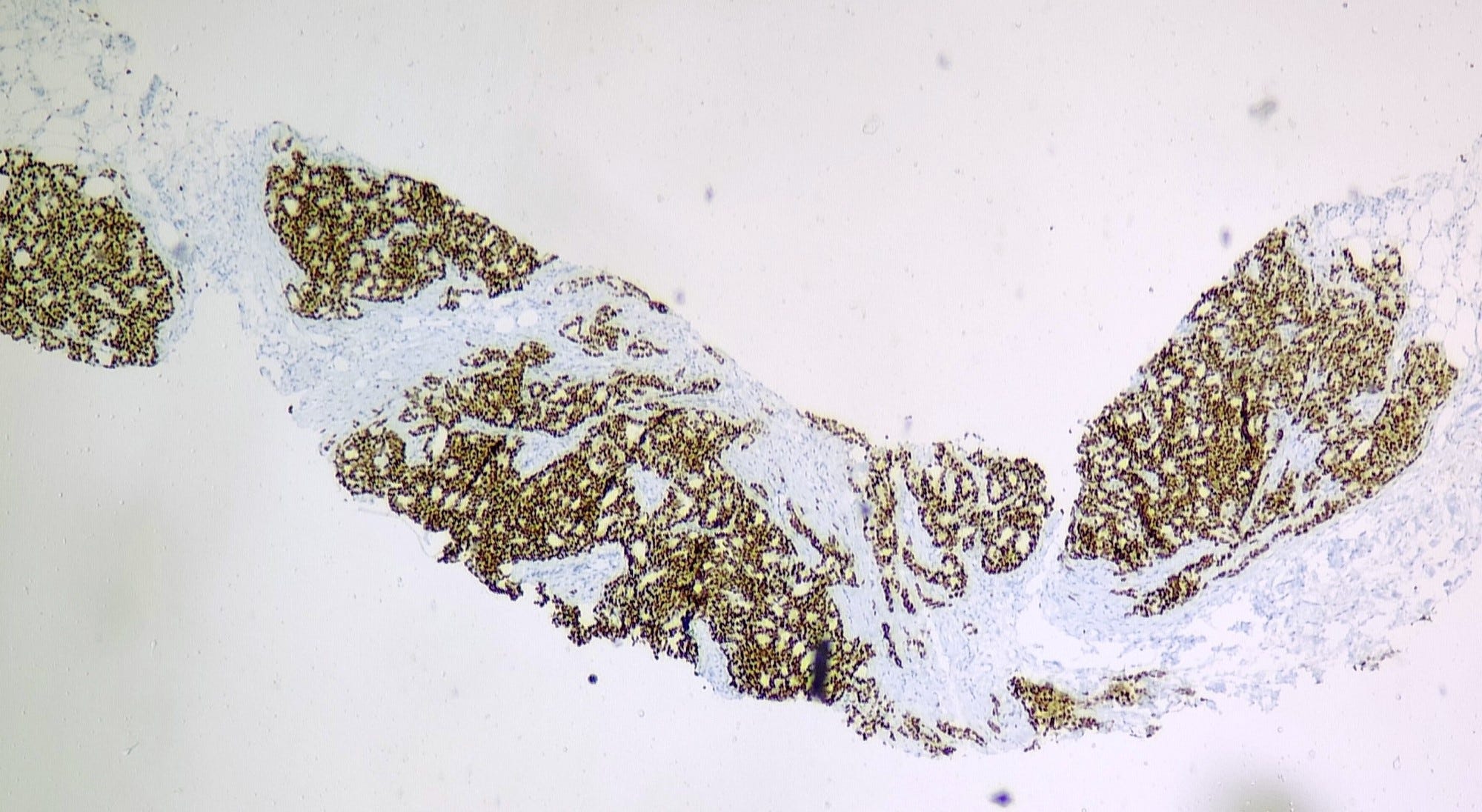
Microscopically, 85% of invasive cancers are poorly differentiated infiltrative ductal carcinoma. DCIS is common - the most common DCIS pattern is papillary, but cribriform, micropapillary and solid patterns are also found.
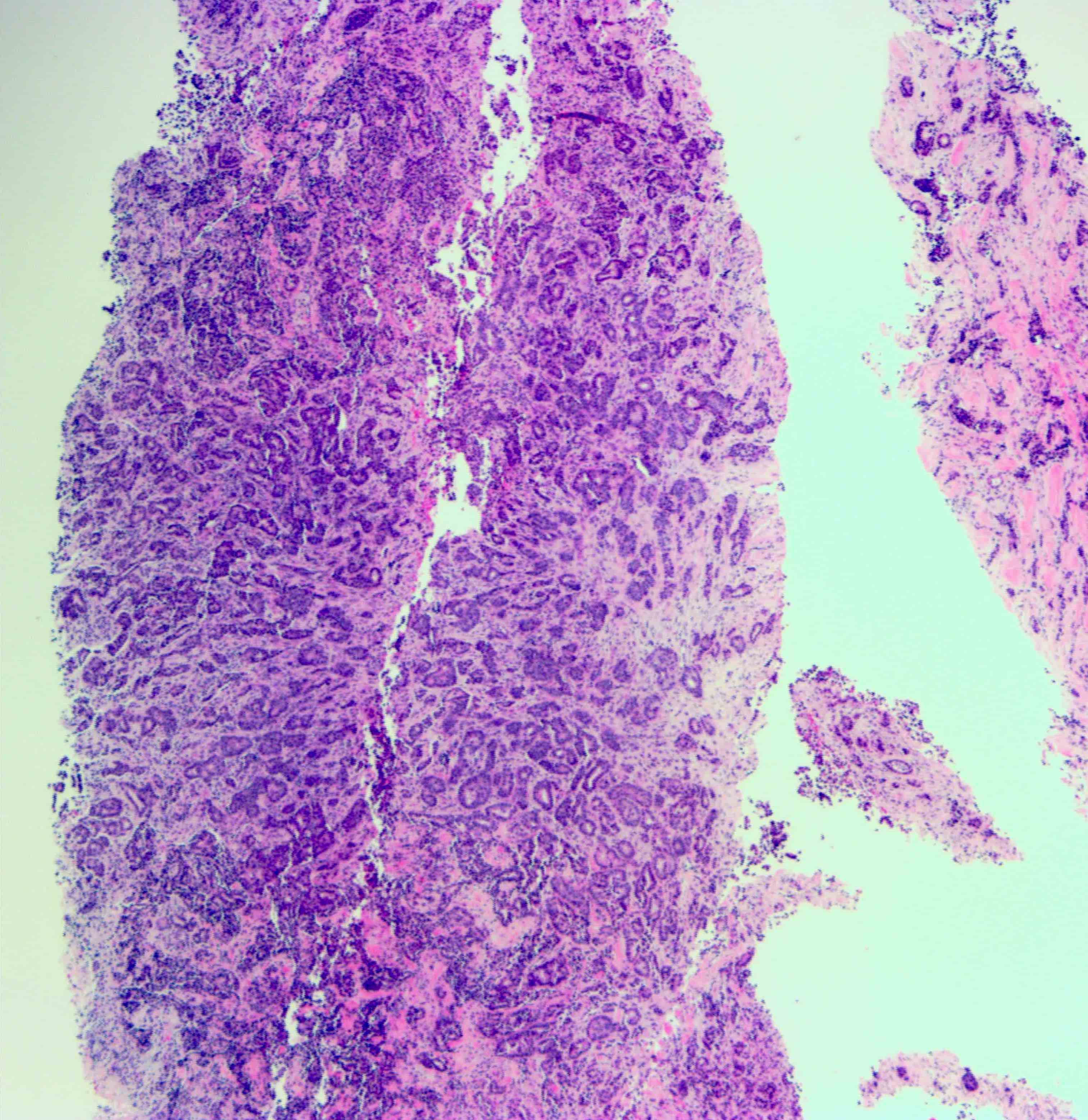
Male invasive breast carcinoma - microscopic images
The next essay, part 6d, will discuss additional breast malignancies with known precursors.
If you like these essays, please subscribe or share them with others.
Click here for the Index to Nat’s blog on Cancer and Medicine.
Follow me at https://www.linkedin.com/in/nat-pernick-8967765/ (LinkedIn), npernickmich (Threads and Instagram), natpernick.bsky.social (Bluesky) or @nat385440b (Tribel).
Follow our Curing Cancer Network through our Curing Cancer Newsletter, on LinkedIn or the CCN section of our PathologyOutlines.com blog. Each week we post interesting cancer related images of malignancies with diagnoses plus articles of interest. Please also read our CCN essays.
Latest versions of our cancer related documents:
American Code Against Cancer (how you can prevent cancer)
Email me at Nat@PathologyOutlines.com - Unfortunately, I cannot provide medical advice.
I also publish Notes at https://substack.com/note. Subscribers will automatically see my Notes.