


My male breast cancer, part 1
5 May 2025, revised 12 July 2025

On 9 April 2025, I underwent a double mastectomy and right sided sentinel node dissection for right sided male breast cancer. This is the first of a series of essays where I share my experience from a pathologist’s perspective.
I have no family history of breast cancer. As described here, back in 1980, I discovered a pelvic lymph node that my physician assessed as benign. I didn’t measure it and wasn’t advised to follow up, but I did periodically check it. In November 1983, I noticed a rock hard, golf ball sized mass near the original node, which I knew was cancer. A biopsy revealed it was Hodgkin lymphoma. I underwent surgery for staging (to determine the extent of disease), followed by radiation therapy to the pelvis, abdomen, chest and lower head and neck.
There is a 23 fold increased risk of breast cancer in men who have received radiation therapy to the chest for Hodgkin lymphoma. However, the incidence remains low at just 0.7% after 40 years.
Since 2000, my doctors have diagnosed me with gynecomastia, or male breast enlargement, though it appeared to be less pronounced than what I’ve observed in other men my age at the beach. It seemed to fluctuate with my weight. In 2000, a breast oncologist colleague ordered a mammogram and ultrasound, both of which were negative.
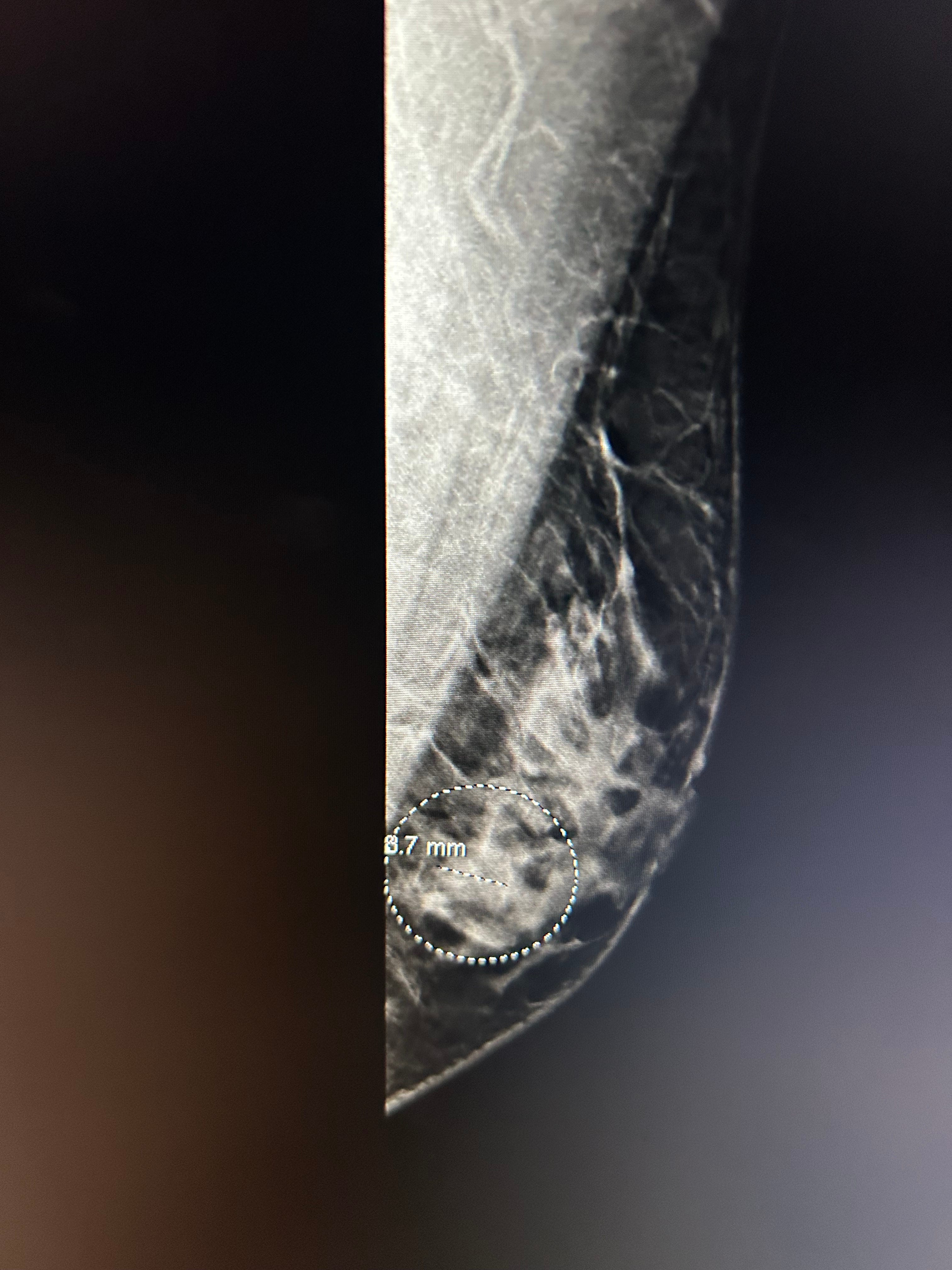
In December 2021, I experienced some rib pain without a known cause. A chest Xray was negative, and I was prescribed Motrin three times a day for seven days. After taking the first pill, the pain resolved. Nevertheless, at my next physical exam, my internist referred me to a breast oncologist. In March 2022, the oncologist felt no mass, but a mammogram revealed “suspicious calcifications” on the left side and the right side was normal. The oncologist didn’t find these calcifications too concerning but suggested followups for 2 years on the left side; these showed stable calcifications and no changes. When I talked to the radiologists about these findings, they indicated it wasn’t normal but didn’t seem too concerned. In November 2022, the oncologist again found no mass on either side. That was the last physical exam until March 2025.
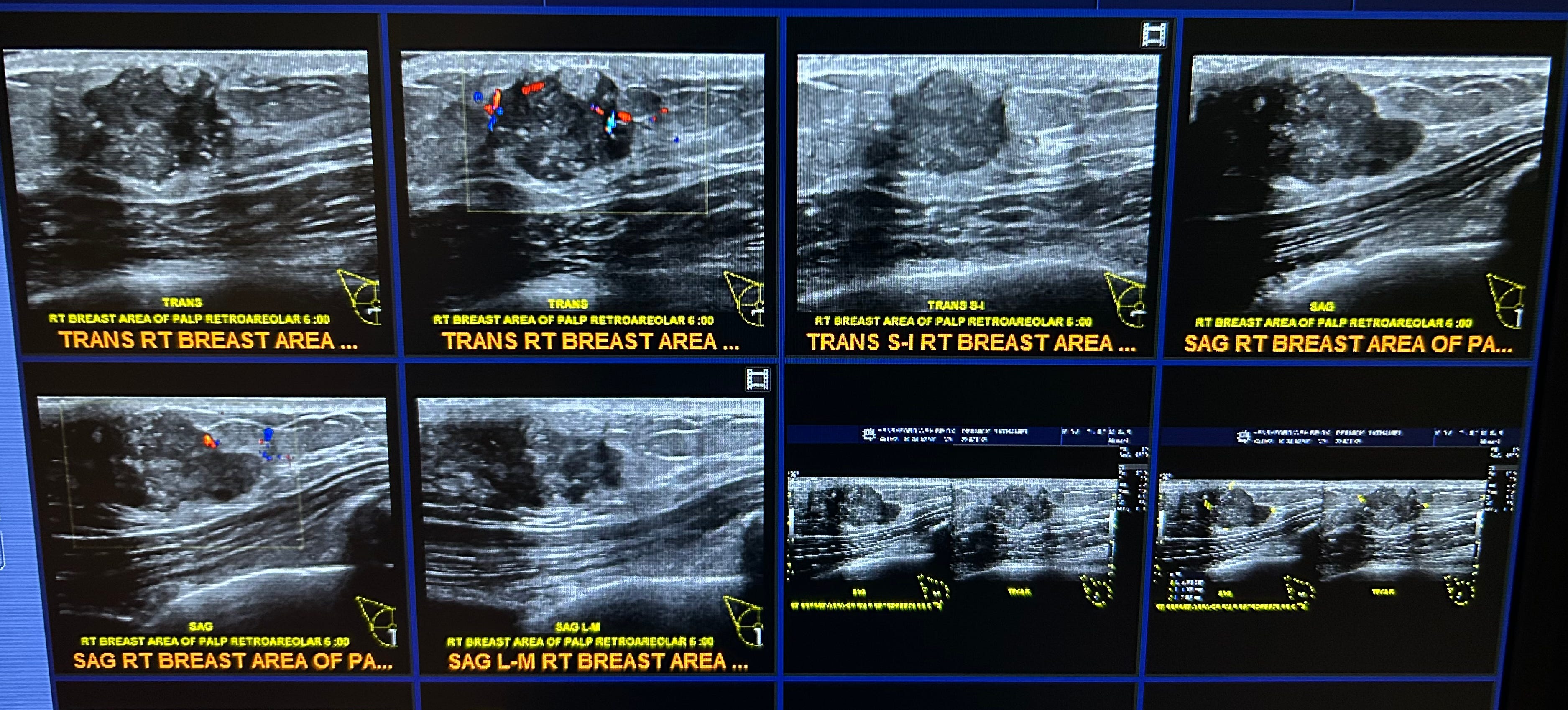
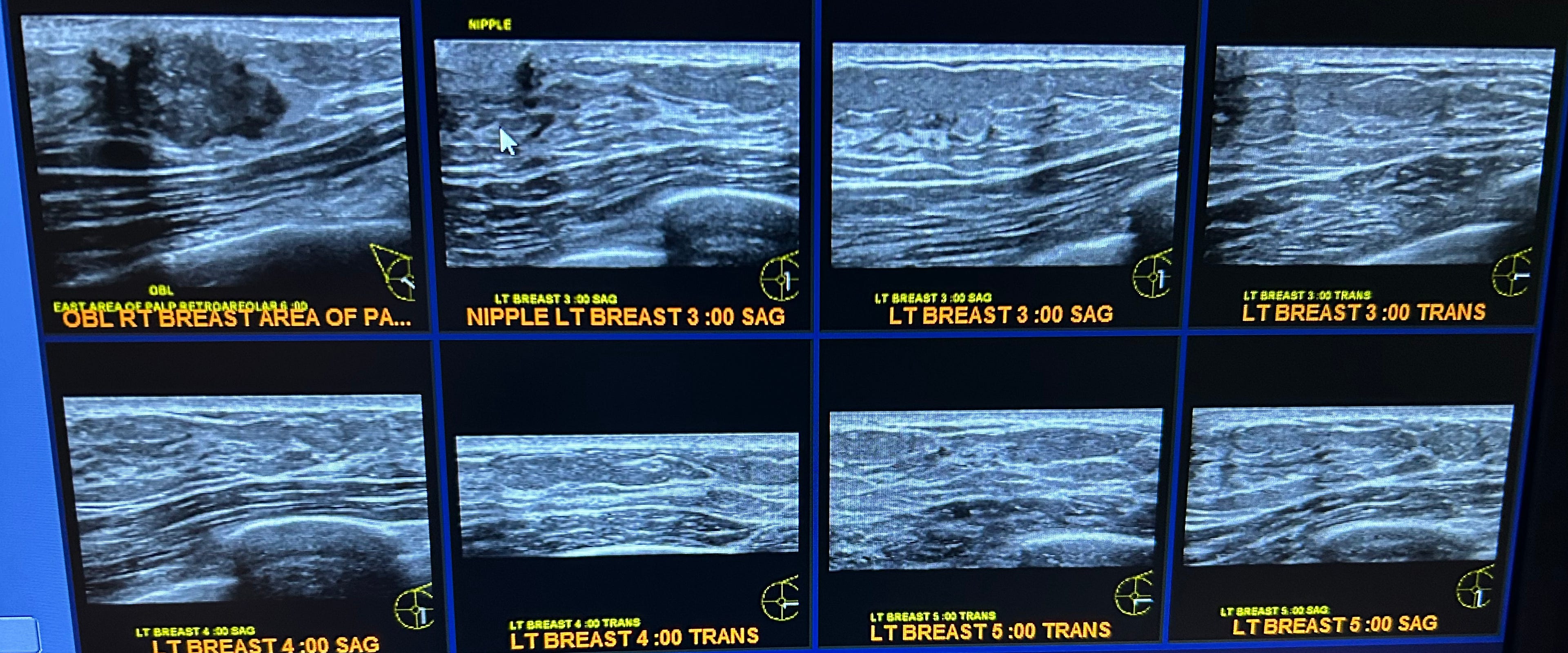
On 13 March 2025, I experienced some right sided chest pain that disappeared after taking Motrin. The following day, I discovered a 2-3 cm, right sided, subareolar breast mass. It was firm, not cystic, and somewhat movable. I immediately contacted my oncologist, and on 19 March 2025, I underwent bilateral mammograms and ultrasounds. On 21 March 2025, I had four ultrasound guided core biopsies on the right side for a 2 cm irregular mass and two core biopsies on the left side for a 0.8 cm mass, which was thought to possibly be fat.
The diagnoses were as follows:
Right breast mass: Invasive ductal carcinoma with micropapillary features, Nottingham grade 3 (high grade). Ductal carcinoma in situ, intermediate nuclear grade, cribriform pattern with comedonecrosis and calcifications.
Estrogen receptor: Strongly positive (99%)
Progesterone receptor: Strongly positive (99%)
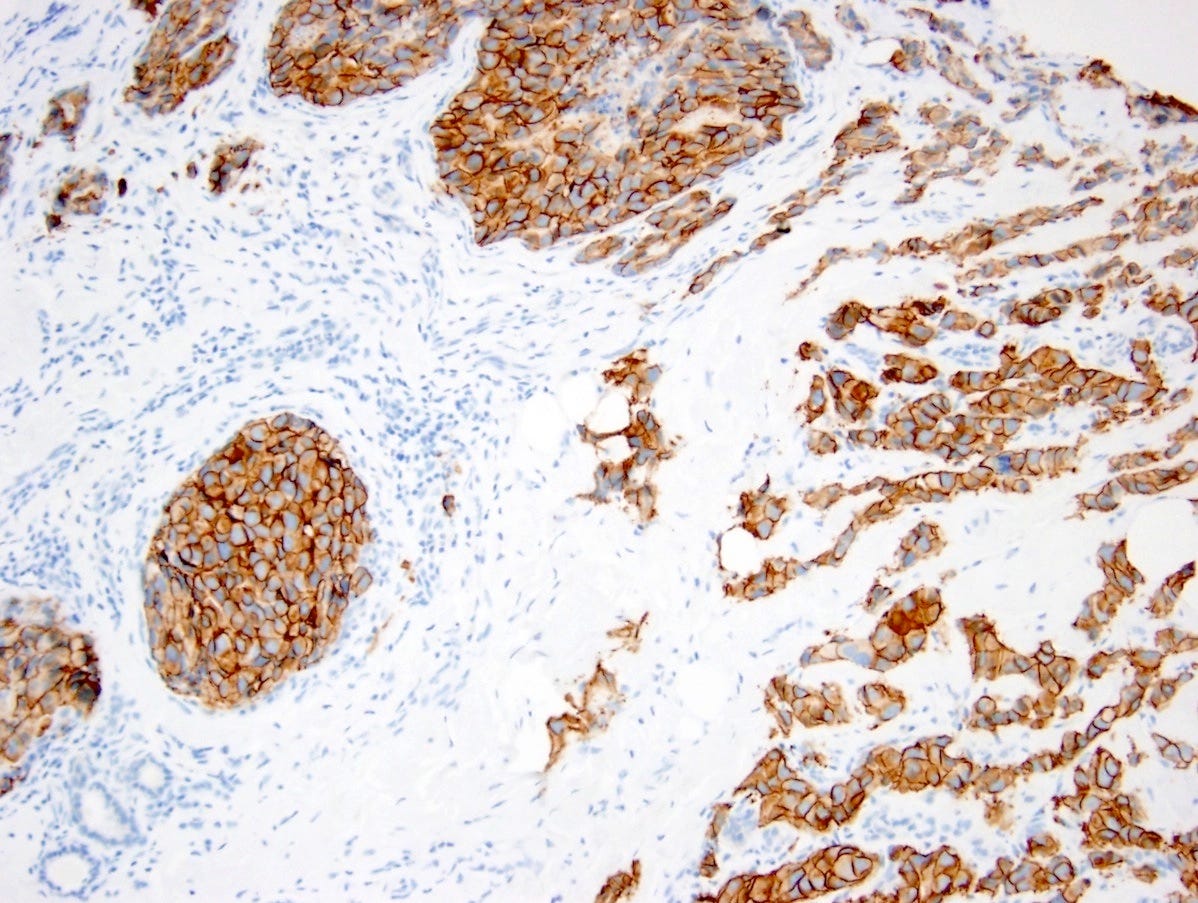
HER2 (immunohistochemistry): 2+ (equivocal), HER2 - FISH: Negative
Ki-67 staining, which measures the rate of cancer cells undergoing mitosis (cell division), was 15%.
2. Left breast ultrasound guided biopsy: Benign fibroadipose tissue. This is discordant and recommend consideration of surgical excision as finding appears masslike on ultrasound.
Microscopic images of the right sided core biopsy are shown below:











The next essay, part 2, will discuss my subsequent double mastectomy.
If you enjoy these essays, please subscribe or share them with others.
Click here for the Index to Nat’s blog on Cancer and Medicine.
Follow me on LinkedIn, Threads and Instagram (@npernickmich) or Bluesky (@natpernick.bsky.social).
Follow our Curing Cancer Network through our Curing Cancer Newsletter, on LinkedIn or in the CCN section of our PathologyOutlines.com blog. Each week we post interesting cancer related images of malignancies with diagnoses plus articles of interest. Please also read our CCN essays.
Latest cancer related documents:
American Code Against Cancer (how you can prevent cancer)
Email: Nat@PathologyOutlines.com (please note I cannot provide medical advice)
Be sure to follow my Substack Notes — subscribers are automatically notified.
Hi Nat, I just read your blog post to my community college English students here in Sacramento, CA. I'm so moved by your story. They're working on making blogs, and yours is an incredible model. Truly, your story is so important. I hope you are feeling okay. I appreciate you!
Thank you Nat for being courageous enough to share your story. As a breast oncologist who writes about the patient experience on Substack I am really interested in your insights.