


Cancer precursor project - breast cancer, part 6d1
4 February 2025
Our cancer precursor project focuses on how different types of cancer arise. Part 6 focuses on breast cancer.
In part 6a, we discussed breast cancer mortality, breast cancer risk factors and how breast cancer arises. In part 6b, we discussed breast anatomy and histology and started our discussion of the 14 invasive breast cancers with known precursors, which continued in part 6c and part 6d. In this essay, we discuss three rare, invasive breast papillary tumors that appear to arise from or be associated with noninvasive but malignant tumors:
Encapsulated papillary carcinoma of the breast with invasion
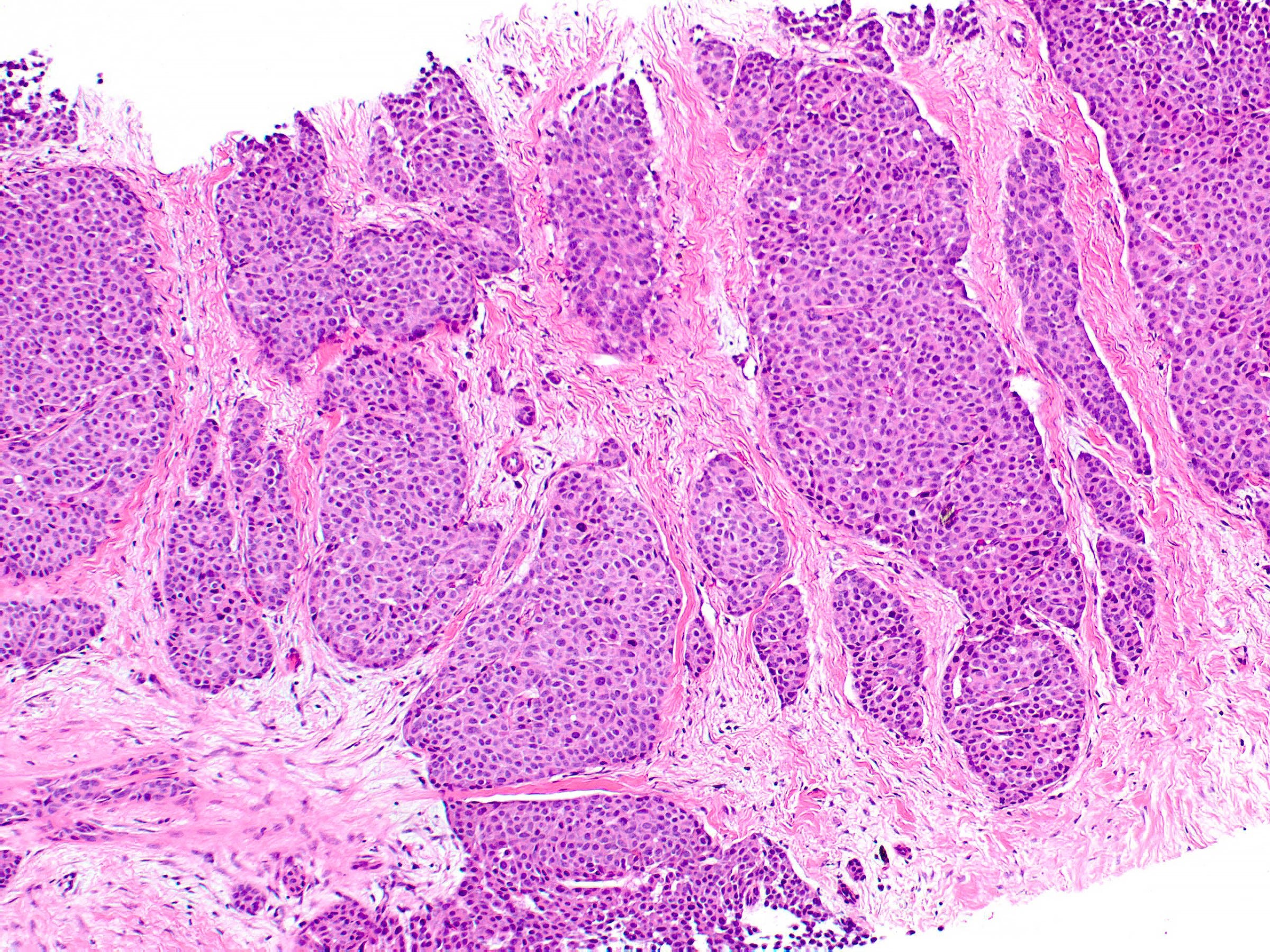
Encapsulated papillary carcinoma without invasion is a rare (0.5 to 1.0% of all breast tumors) papillary breast tumor of postmenopausal women consisting of delicate papillary fronds with fibrovascular cores. The fronds are typically lined by cuboidal to columnar epithelial cells with low to intermediate atypia, often within a cystically dilated duct surrounded by a thick fibrous capsule. The tumors are typically ER+, PR+ and HER2-. They behave and are staged comparable to ductal carcinoma in situ (DCIS) and have an excellent prognosis.
Although staged as DCIS and not actually invasive, encapsulated papillary carcinoma has features of an indolent invasive carcinoma, not DCIS:
The capsule arises from a reactive process and is not a thickened basement membrane.
The tumor lacks myoepithelial cells along the papillae and around the periphery of the tumor or has only focal peripheral myoepithelial staining, which is characteristic of invasive carcinoma.
In 3% of cases, encapsulated papillary carcinoma has malignant features of high grade cytologic atypia and increased mitotic activity, with variable invasion of tumor cells beyond the fibrous capsule. These cases are classified and staged as a high grade invasive breast carcinoma with features of encapsulated papillary carcinoma, even if they are not actually invasive. They have an excellent prognosis, comparable to cases without malignant features.
How encapsulated papillary carcinoma arises from normal breast tissue or transforms into a tumor resembling invasive carcinoma is unknown. It has a characteristic recurrent somatic mutation of ZFPM1, a chromatin modification gene, as well as mutations of genes in the PI3K-AKT-mTOR pathway. The genomic profiles of encapsulated, solid and invasive papillary carcinoma are similar and resemble those of low grade, ER+ breast cancers with low numbers of gene copy number aberrations or p53 alterations.
Surgical excision appears to be adequate treatment, similar to DCIS. Hormonal treatment may be indicated in ER+ cases. Chemotherapy is not indicated. Axillary sentinel nodal sampling may not be indicated. There is no consensus on the use of radiation therapy.
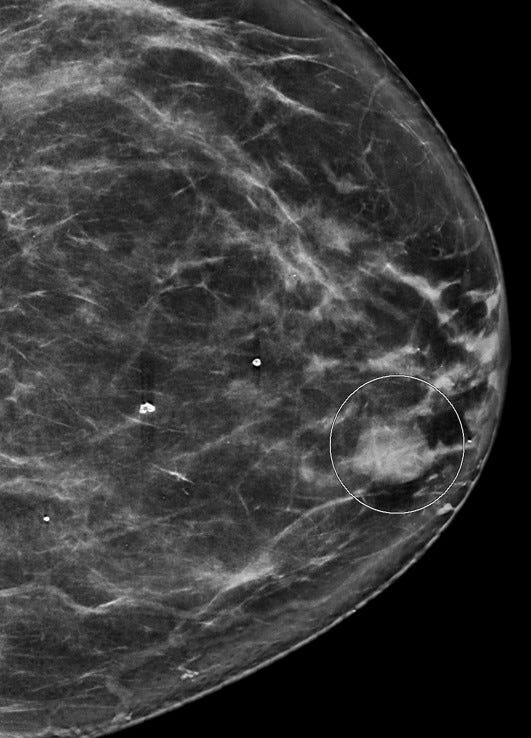
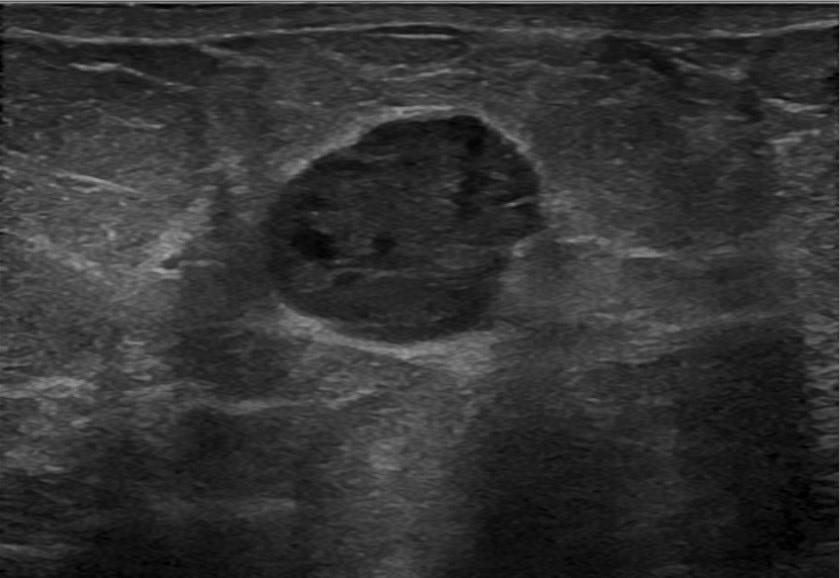
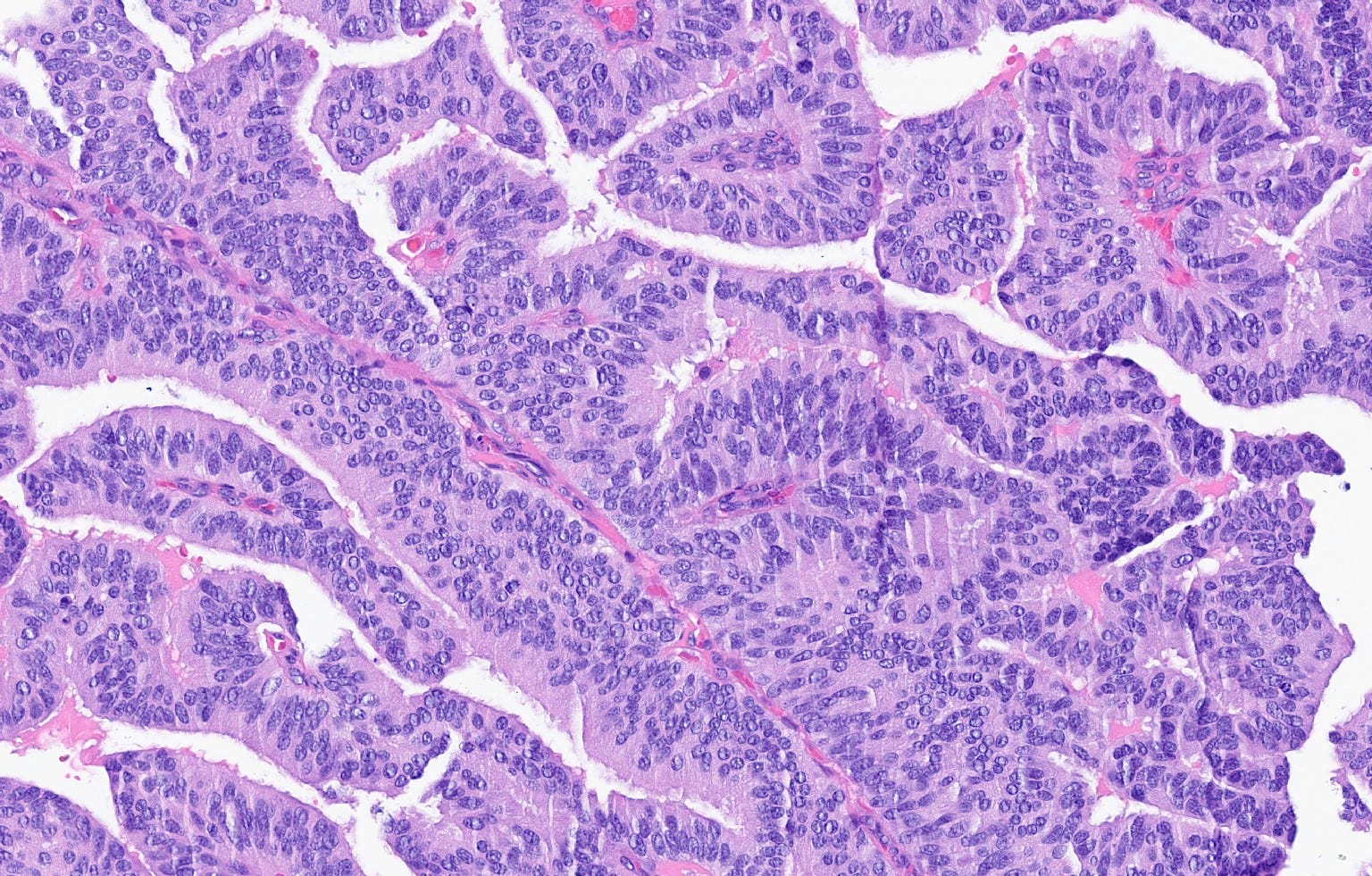
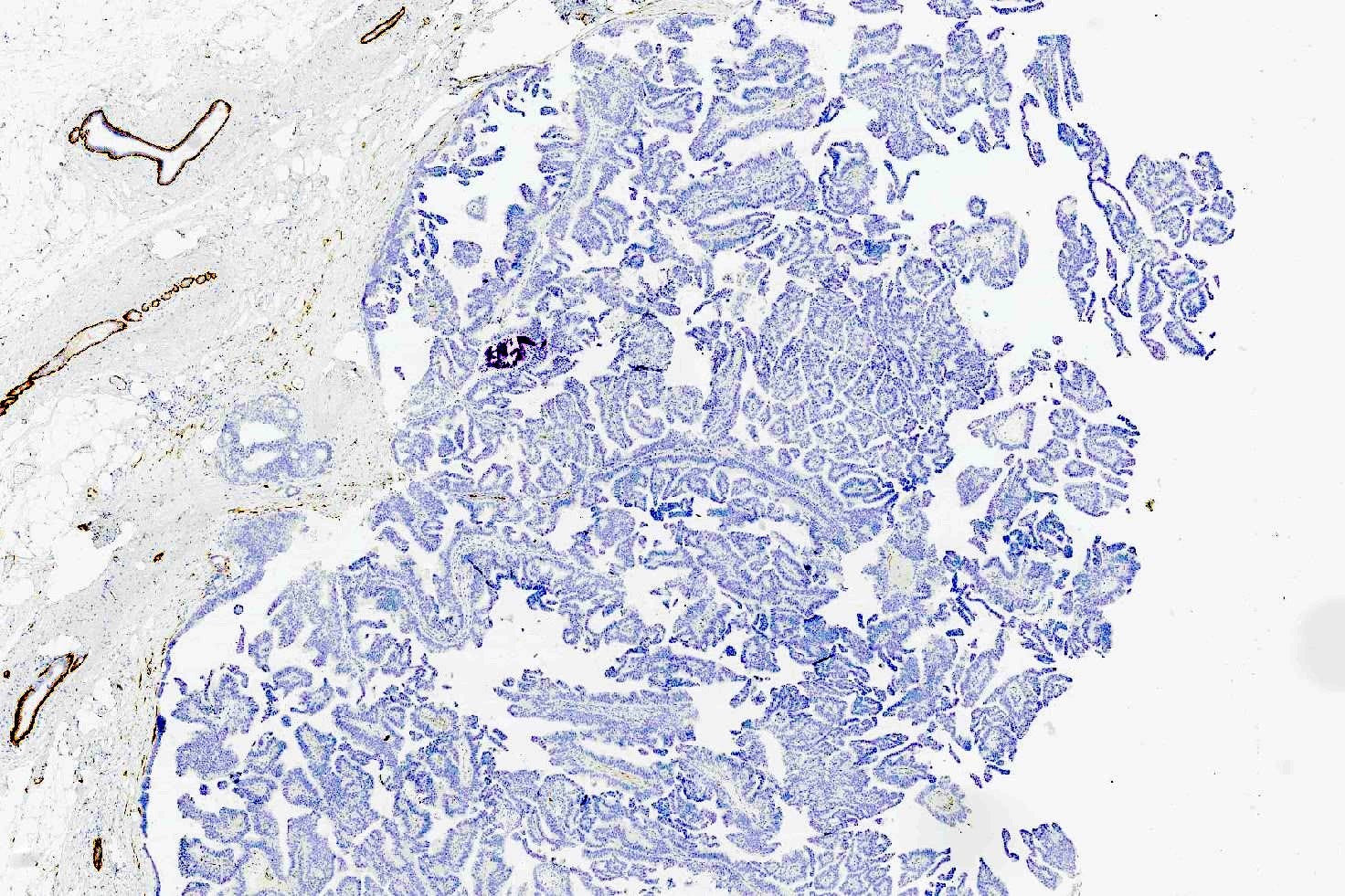
Encapsulated papillary carcinoma of the breast - radiologic and microscopic images
Solid papillary carcinoma of the breast with invasion
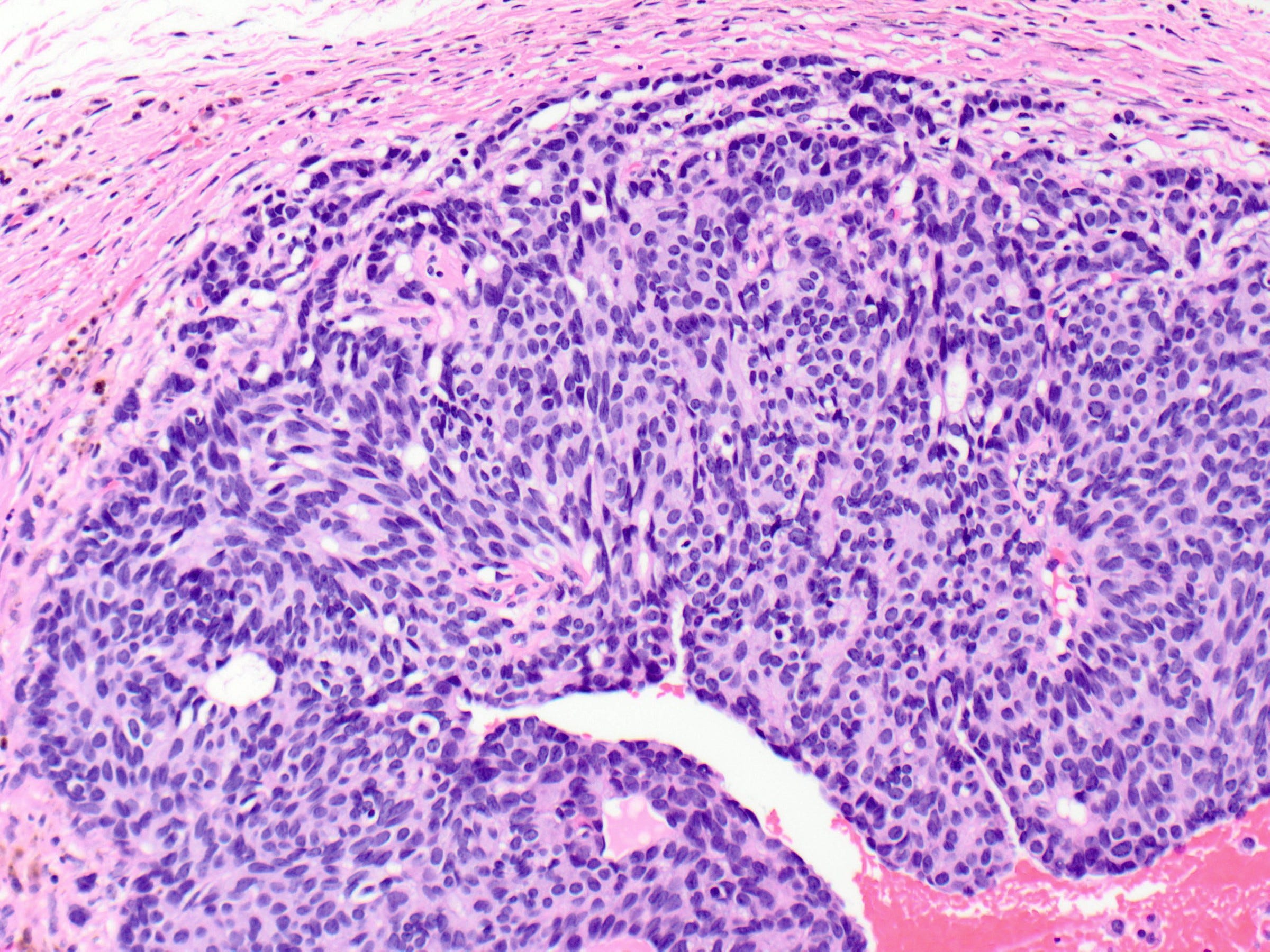
Solid papillary carcinoma of the breast (with or without invasion) is a rare subtype (< 1% of breast carcinomas) of infiltrating ductal carcinoma. It typically occurs in post menopausal women and is characterized by a circumscribed solid growth pattern with interspersed delicate fibrovascular cores. The cells have low or intermediate grade nuclear atypia. Neuroendocrine differentiation is common.
Solid papillary carcinoma of the breast may be in situ or invasive. In situ carcinoma is diagnosed when the tumor has well circumscribed solid nests; myoepithelial cells may or may not be demonstrable at the periphery. Invasive carcinoma is diagnosed when there is a convincing pattern of infiltrative growth and no myoepithelial cells. Both types are ER+ and HER2- and have a genomic profile that resembles other low grade, ER+ breast cancers with low numbers of gene copy number aberrations or p53 alterations. They have a higher expression of genes related to neuroendocrine differentiation and a recent report suggests they may be comparable to neuroendocrine tumors at other sites. They have an excellent prognosis.
Solid papillary carcinoma in situ may transform into either solid papillary carcinoma with invasion or infiltrating ductal carcinoma with neuroendocrine differentiation.
In situ cases are treated similarly to DCIS. Invasive carcinoma cases are treated similarly to infiltrating ductal carcinoma.
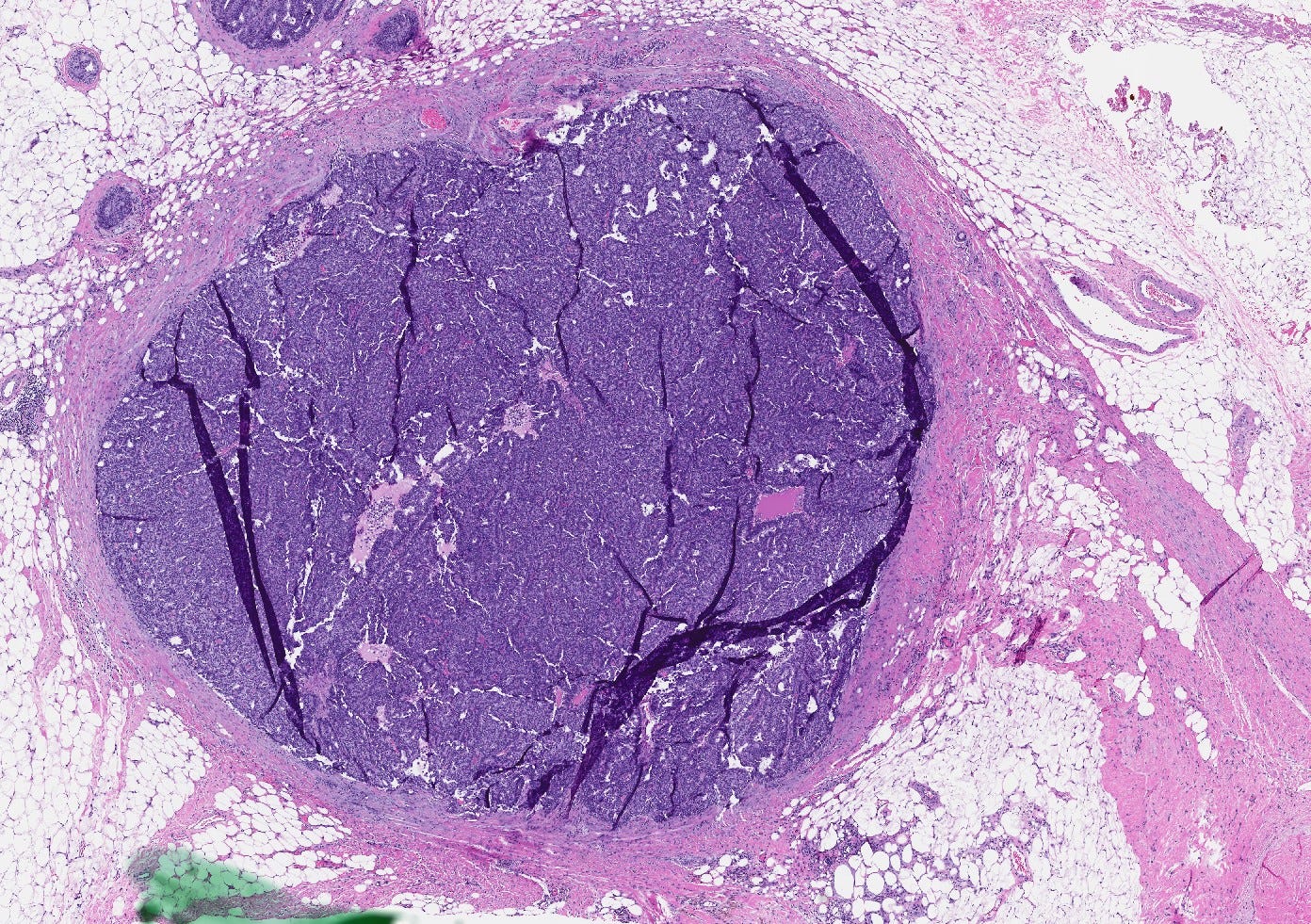
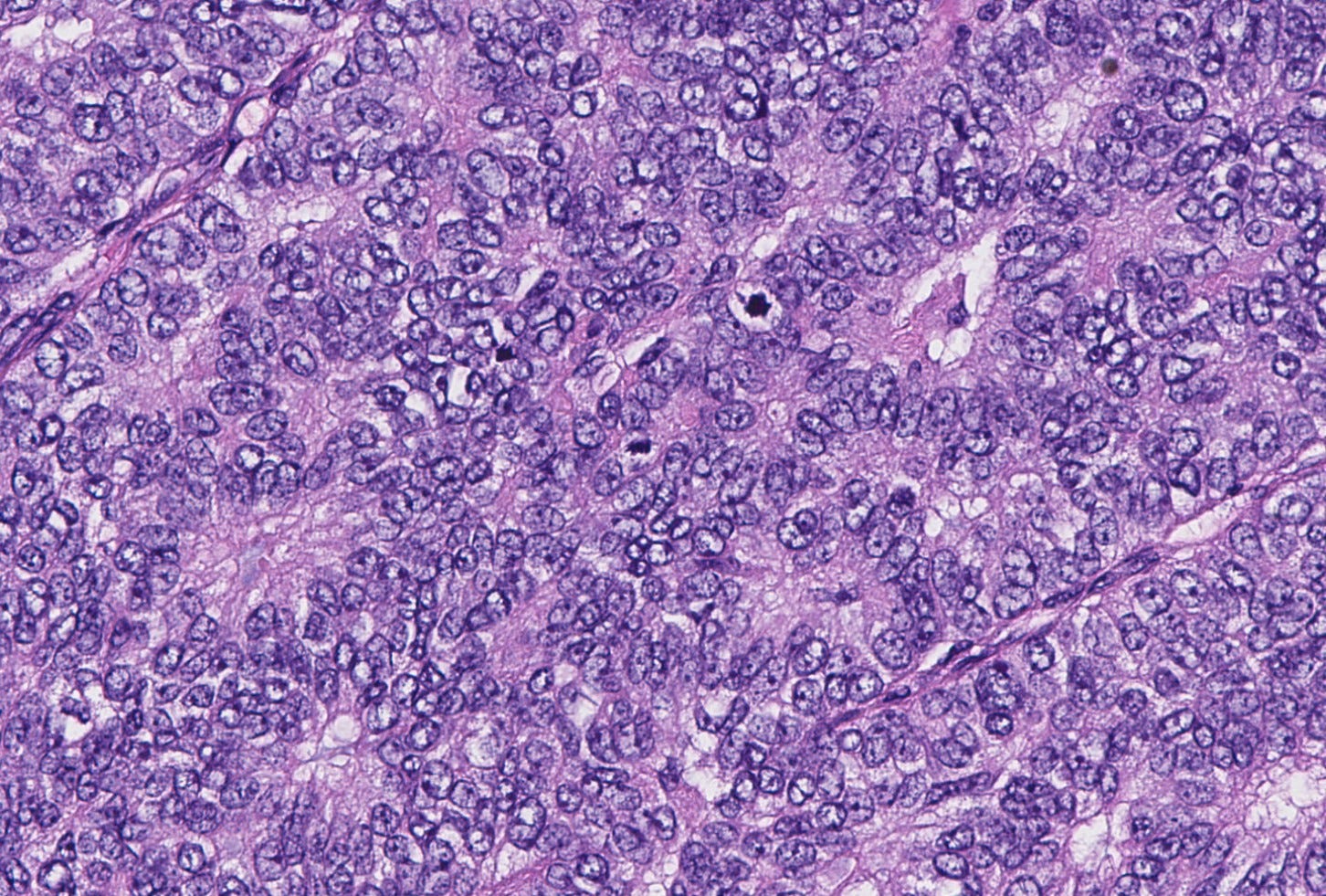
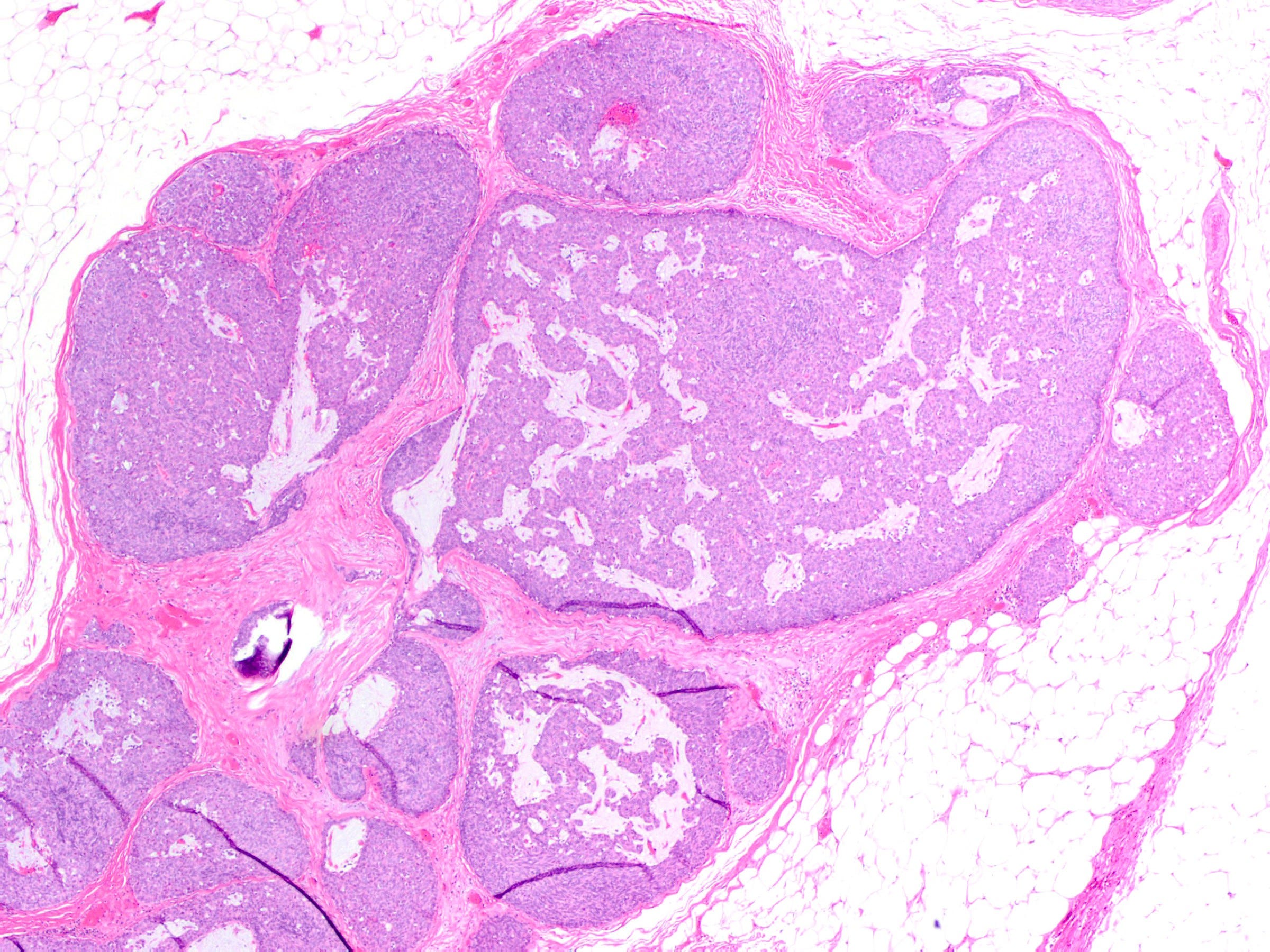
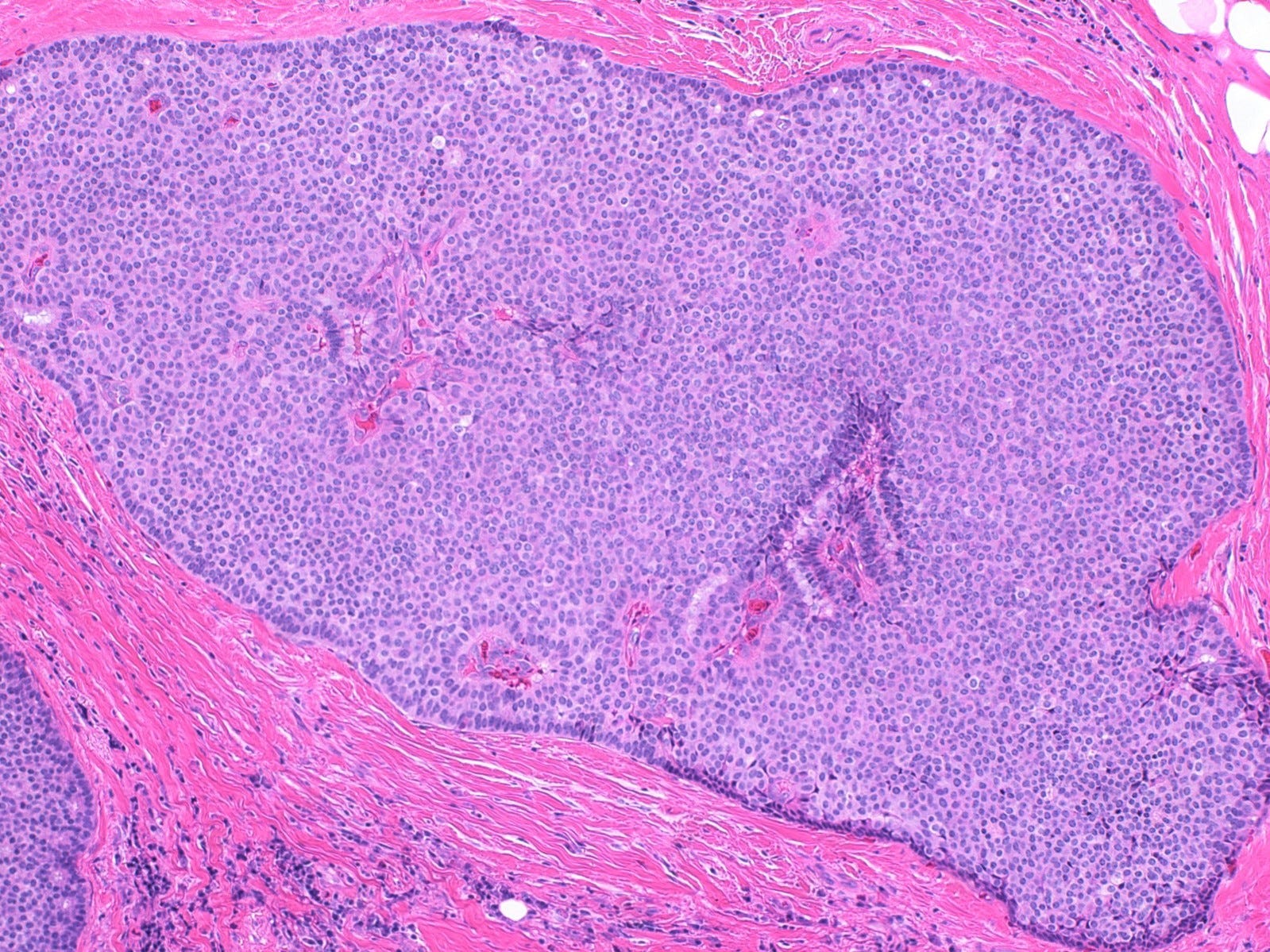
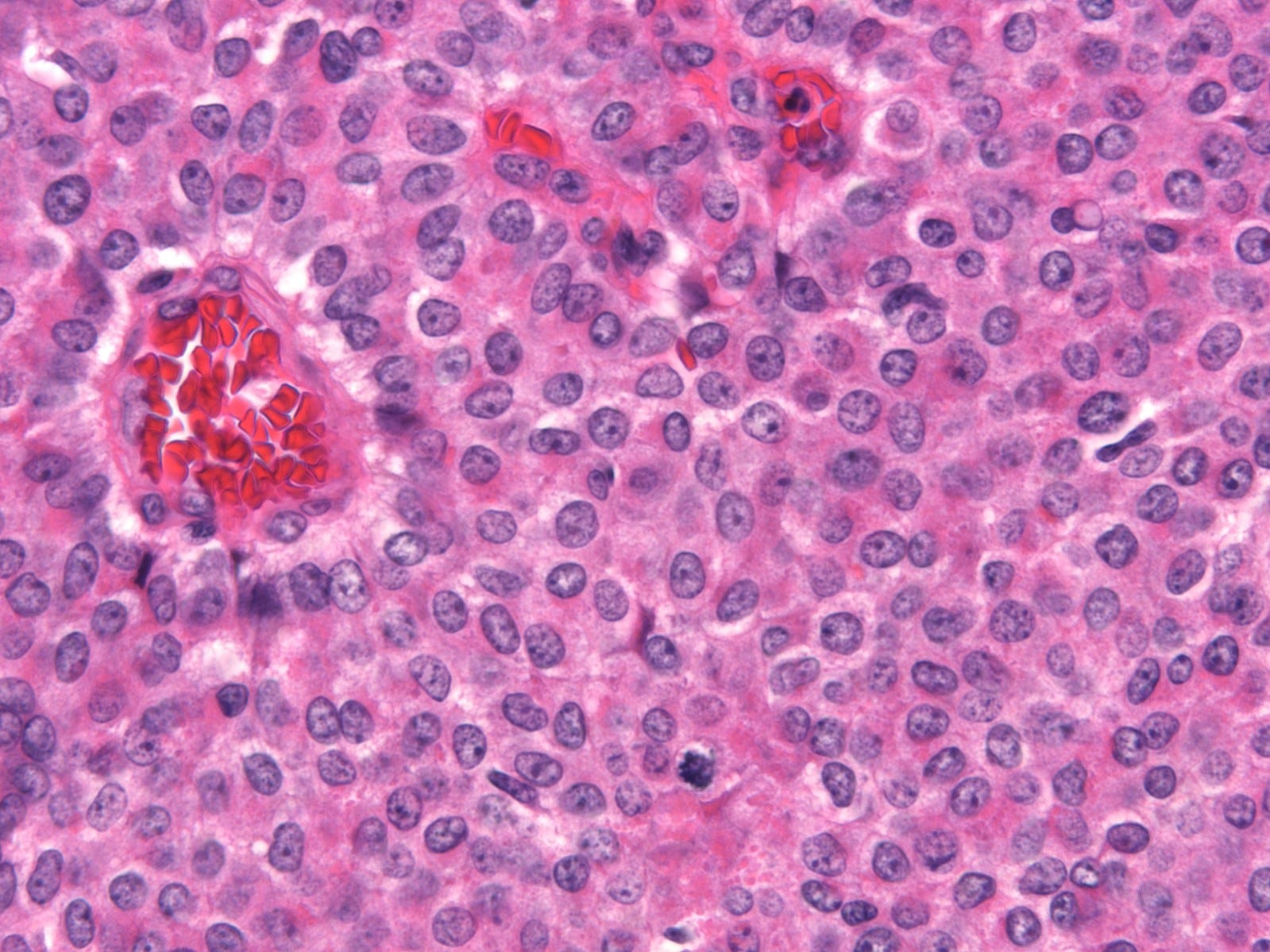
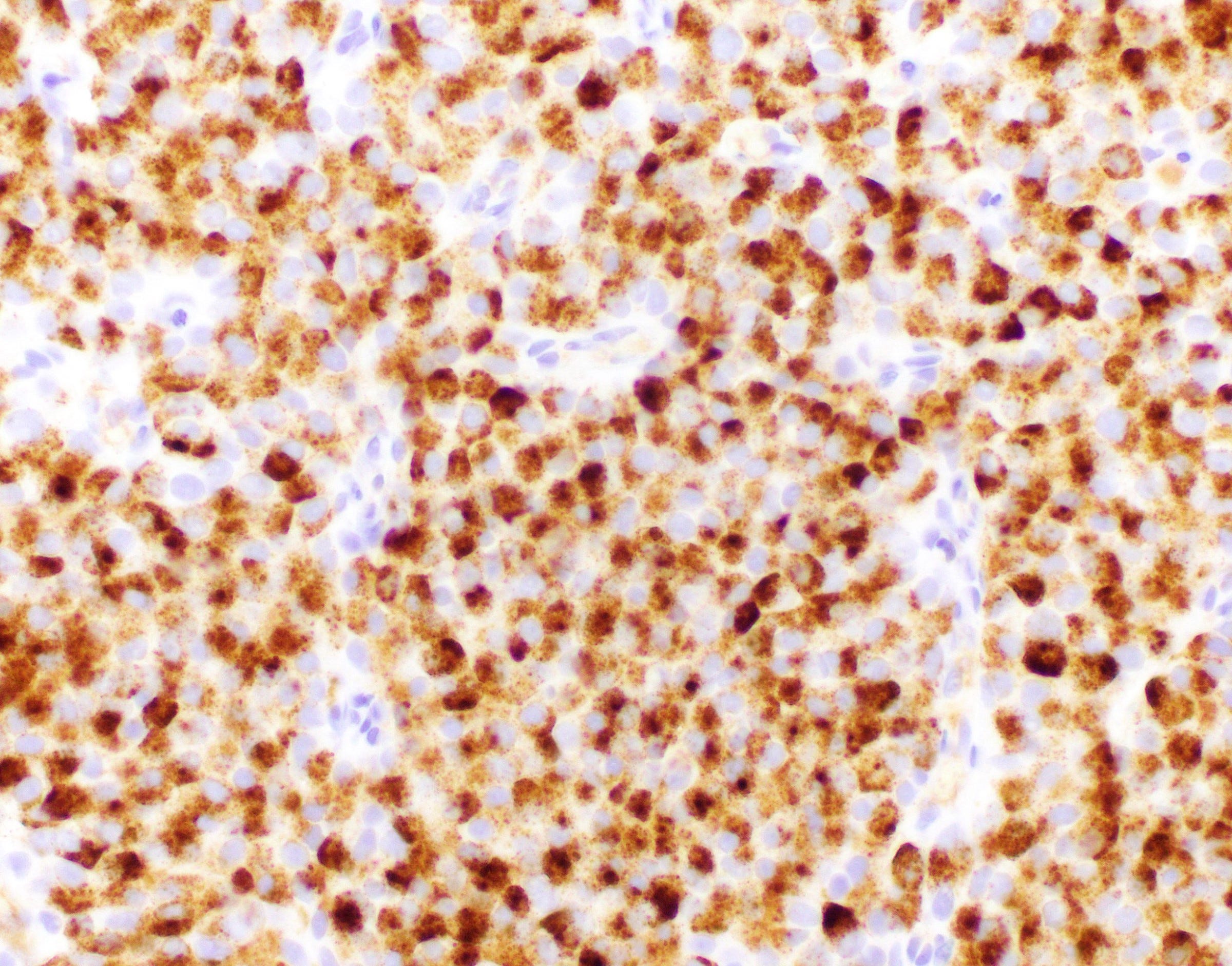
Solid papillary carcinoma of the breast - gross and microscopic images

Intraductal papillary carcinoma of the breast with invasion
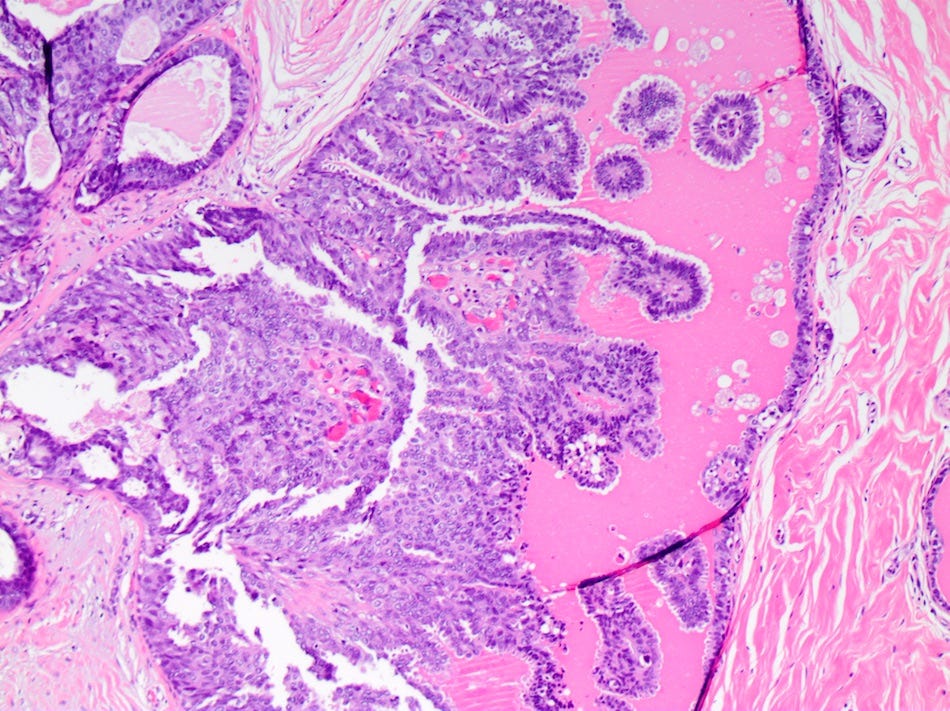
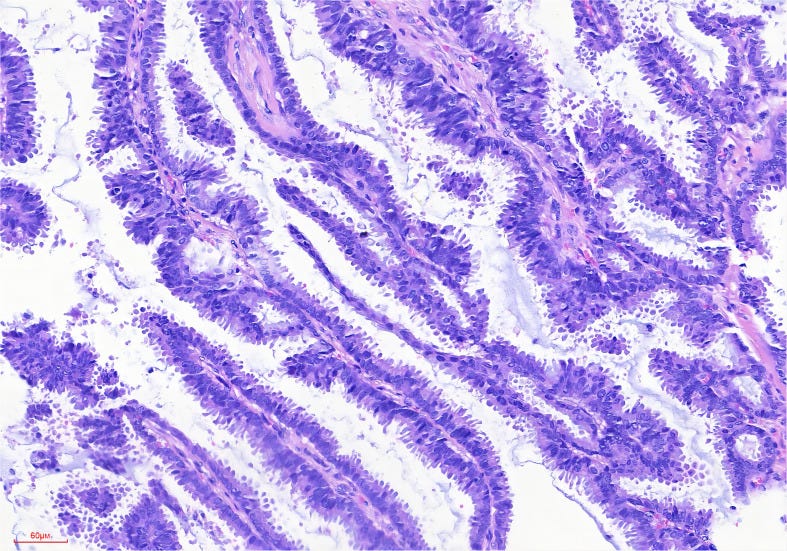
Intraductal papillary carcinoma with invasion (also called intraductal papillary adenocarcinoma with invasion or papillary DCIS with invasion) is a rare breast cancer (0.5% of all invasive breast cancers) that is part of the WHO classification of breast cancers. It is an invasive adenocarcinoma with more than 90% papillary structures in the invasive component. It has a dendritic fibrous vascular core lined with layered columnar epithelial cells but lacks a complete myoepithelial layer in the papilla. Lymph node metastases may occur in 20% of patients.
There is no established optimal treatment other than surgery, due to insufficient research.
Traditionally these patients are considered to have a high survival rate (probability of death due to disease of only 1.4% within 5 years and 5.4% within 10 years) but another study claims a prognosis similar to infiltrating ductal carcinoma.
Intraductal papillary carcinoma with invasion appears to arise from papillary DCIS, which consists of papillary fronds containing prominent fibrovascular septa projecting into the duct lumen; its papillary cores generally lack a myoepithelial cell layer. Papillary DCIS may undergo malignant transformation due to mutations in the TP53 gene (typically a deletion) and in PIK3CA and AKT genes.
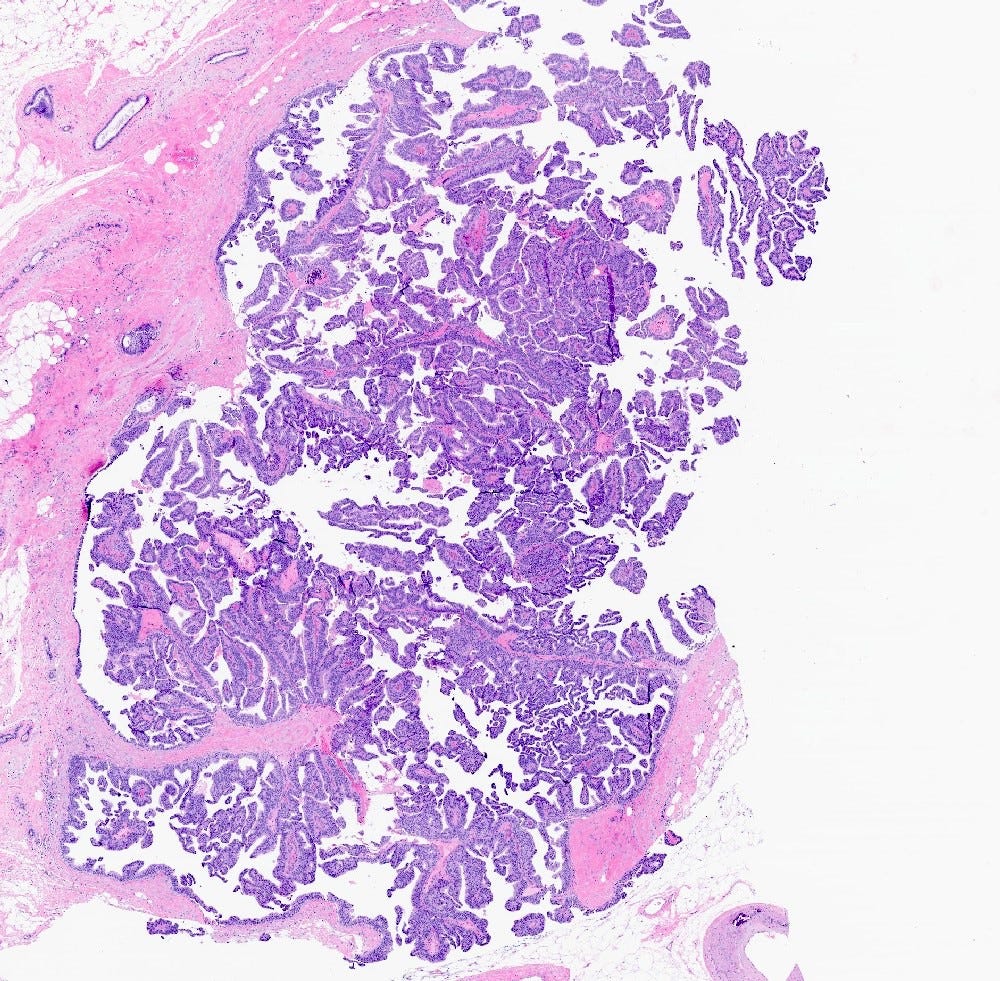
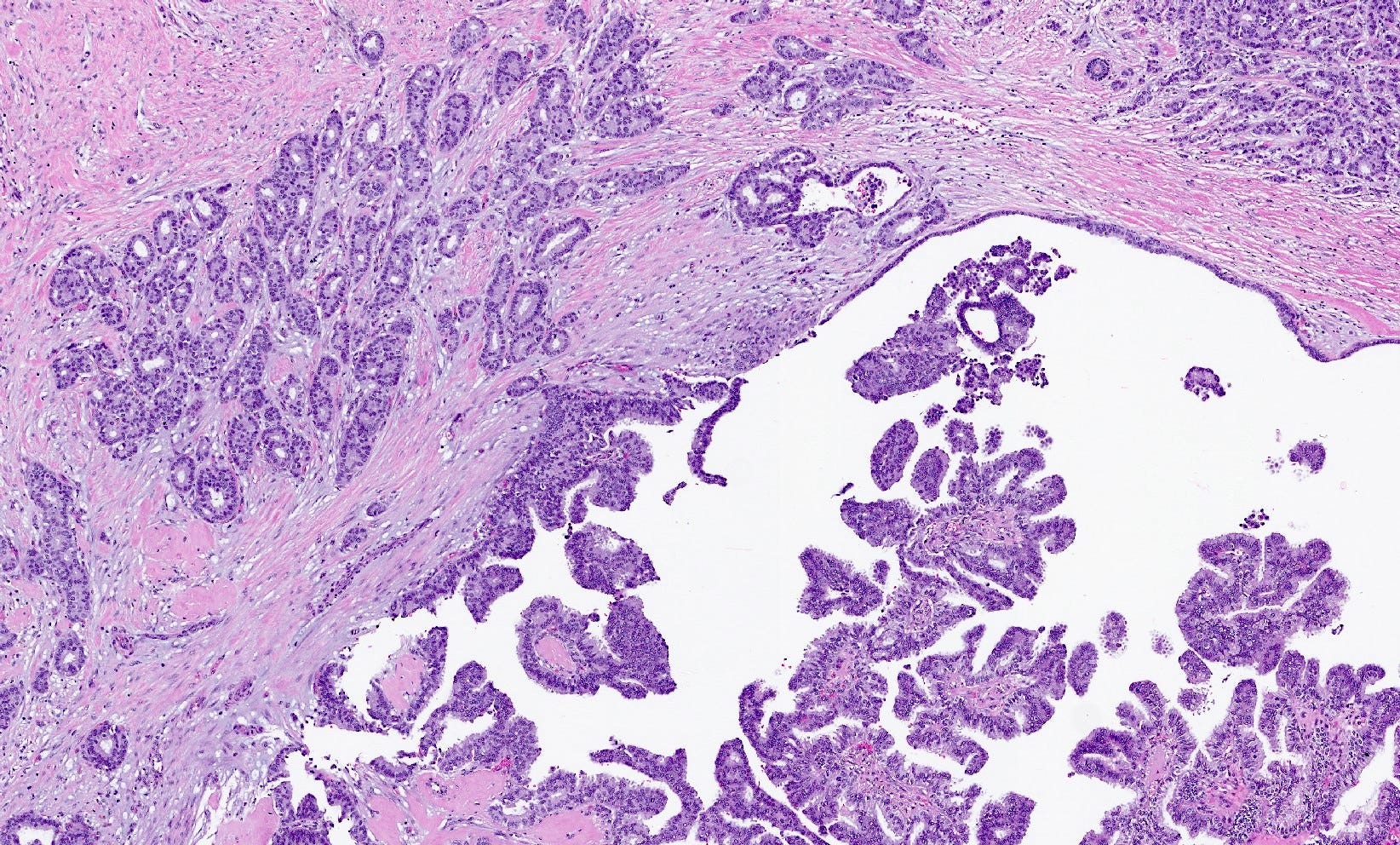
Intraductal papillary adenocarcinoma of the breast with invasion - microscopic images
The next essay, part 6e, will begin our discussion of breast malignancies with no known precursors beginning with BRCA associated carcinoma.
If you like these essays, please subscribe or share them with others.
Click here for the Index to Nat’s blog on Cancer and Medicine.
Follow me at https://www.linkedin.com/in/nat-pernick-8967765/ (LinkedIn), npernickmich (Threads and Instagram), natpernick.bsky.social (Bluesky) or @nat385440b (Tribel).
Follow our Curing Cancer Network through our Curing Cancer Newsletter, on LinkedIn or the CCN section of our PathologyOutlines.com blog. Each week we post interesting cancer related images of malignancies with diagnoses plus articles of interest. Please also read our CCN essays.
Latest versions of our cancer related documents:
American Code Against Cancer (how you can prevent cancer)
Email me at Nat@PathologyOutlines.com - Unfortunately, I cannot provide medical advice.
I also publish Notes at https://substack.com/note. Subscribers will automatically see my Notes.