


Cancer precursor project - summary as of 18 July 2024
This project started in January 2024. Our findings to date are shown below:
We have identified 1218 distinct human malignancies (the number changes slightly over time as we review each malignancy). Our definitions of distinct and malignancy are here.
Although precursor refers to tissue antecedents of cancer, pathologists occasionally use a broader definition based on clinical findings. For example, MGUS and B cell monoclonal lymphocytosis are considered precursors of myeloma and CLL / SLL, respectively, but the precursors have the same morphology as the malignancy; they differ only in clinical findings.
Cancer precursors are not universal, as was previously thought (Caporaso 2013). Even using our broader definition, only 14.3% of malignancies have a known precursor.
The presence of precursors varies by subspecialty (data as of 12 July 2024):
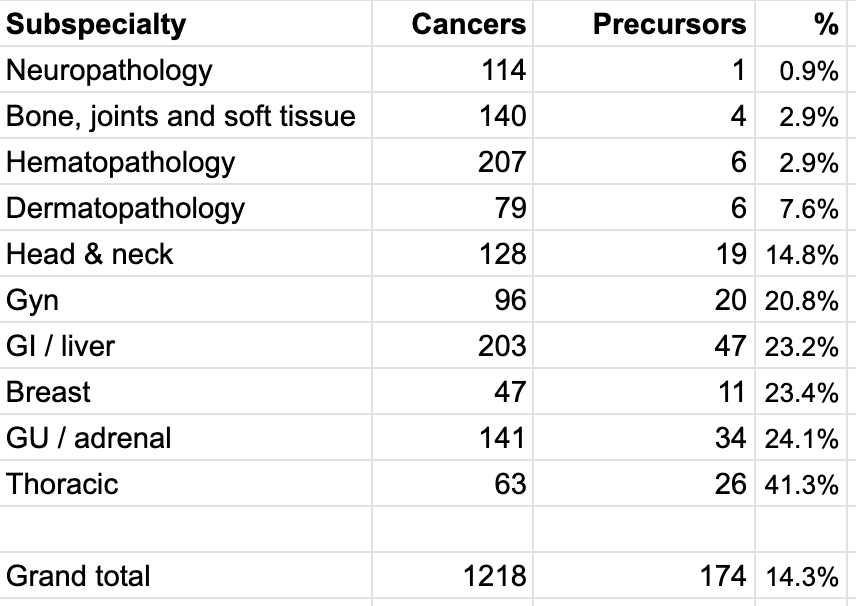
Nonepithelial malignancies only rarely have precursors and even then, they are typically rare, associated with genetic syndromes or based on clinical and not morphologic findings:
Neuropathology: none of the 100 CNS malignancies have known precursors. Only 1 of 14 eye malignancies has a precursor: conjunctival squamous cell carcinoma, an epithelial lesion, has conjunctival intraepithelial neoplasia as a precursor.
Bone, joints and soft tissue: none of 104 soft tissue malignancies have known precursors. Only 4 of 36 bone & joint malignancies have precursors and then only rarely: atypical cartilaginous tumor / chondrosarcoma grade 1 (a) and chondrosarcoma, grades 2 & 3 (b) both rarely have enchondroma or osteochondroma as precursors; osteosarcoma, NOS / conventional osteosarcoma (c) and giant cell tumor of bone, malignant (d) both rarely have Paget disease of bone as precursors.
Hematopathology: only 6 of 207 malignancies have known precursors. As noted, myeloma and CLL / SLL have MGUS and B cell monoclonal lymphocytosis as precursors, but the precursors have the same morphology as the malignancies and differ only in clinical findings. Occasionally, lymphoplasmacytic lymphoma has MGUS IgM as a precursor, also based only on clinical findings. Follicular neoplasia in situ and in situ mantle cell neoplasia are only rarely precursors of follicular lymphoma and mantle cell lymphoma and typically do not progress. In contrast, enteropathy associated T cell lymphoma (EATL) has a classic precursor: celiac disease is a major risk factor for EATL and has different histology, specifically villous atrophy and increased intraepithelial T lymphocytes.
Dermatopathology: only 6 of 79 distinctive skin malignancies have known precursors. Invasive melanoma (a) and superficial spreading melanoma (low CSD [cumulative sun damage] melanoma) (b) both have a precursor of dysplastic nevus. Lentigo maligna melanoma (c) has a precursor of lentigo maligna. Acral melanoma (d) has precursors of acral lentiginous melanoma in situ and acral nevus. Melanoma arising in giant congenital nevus (e) has a precursor of giant congenital nevus. Squamous cell carcinoma (f) has precursors of actinic keratosis / keratinocytic dysplasia and squamous cell carcinoma in situ.
We speculate that malignancies arise through two or possibly three distinct pathways:
First, many malignancies are initiated by a defining mutation or genetic change in a single stem or progenitor cell that multiplies and acquires additional malignant properties. Over time, cell clusters grow in size but form no distinct precursors.
Second, many epithelial or melanocytic malignancies have precursor lesions. This may be due to epithelial cell-cell interactions and basement membranes, which limit inappropriate cell division and invasion of epithelial cells or the keratinocytes they surround unless additional DNA changes are present.
Third, we speculate but have not proven that some epithelial malignancies have a precursor with distinct molecular patterns but no morphologic changes, analogous to malignancies that resemble normal tissue but have distinct molecular changes.

Our next essays will focus on epithelial malignancies with known precursors.
Please subscribe or share these free essays with others. We have an Index to Nat’s blog on Cancer and Medicine
Follow us on Substack, LinkedIn, Threads and Instagram (npernickmich) or Tribel (@nat385440b).
Follow our Curing Cancer Network through our Curing Cancer Newsletter, on LinkedIn or Twitter or the CCN section of our PathologyOutlines.com blog. Each week we post interesting cancer related images of malignancies with diagnoses plus articles of interest. Please also read our CCN essays.
Latest versions of our cancer related documents:
Strategic plan to substantially reduce cancer deaths (June 2023)
American Code Against Cancer (how you can prevent cancer) (January 2023)
Cancer Precursor Project spreadsheet (July 2024) and General Overview (July 2024)
Email me at Nat@PathologyOutlines.com. Unfortunately, I cannot provide medical advice.
I also publish Notes at https://substack.com/note. Subscribers will automatically see my Notes.